
What if surgery could become steadier than the human hand?
Microsurgery is already one of the most technically demanding fields in medicine.
It involves operating on extremely small structures such as blood vessels, lymphatic channels, nerves, tiny ducts, and delicate reconstructive tissues under magnification. These structures may be only a few millimetres wide — or even smaller in supermicrosurgery.
At this scale, surgery becomes more than skill. It becomes a battle against the natural limits of the human hand.
Even expert surgeons have physiological tremor. Long procedures can cause fatigue. Working under a microscope can strain the neck, shoulders, back, eyes, and hands. Tiny movements that would not matter in routine surgery can become important when repairing a small vessel or connecting a fragile lymphatic channel.
This is where robotic microsurgery becomes one of the most exciting frontiers in precision surgery.
The goal is not to replace the microsurgeon. The goal is to amplify the microsurgeon.
Robotic microsurgery uses robotic systems to filter tremor, scale movement, improve precision, enhance ergonomics, and help surgeons work in tiny anatomical spaces with greater control.
The real idea is simple: Robotic microsurgery turns human intention into digitally refined microsurgical movement.

- Microsurgery is not simply “small surgery.”
- It is surgery where the target structures are so delicate that precision directly affects survival, healing, and function.
- Robotic microsurgery enters the field because it supports the exact things that make microsurgery difficult: steadiness, scale, precision, and endurance.
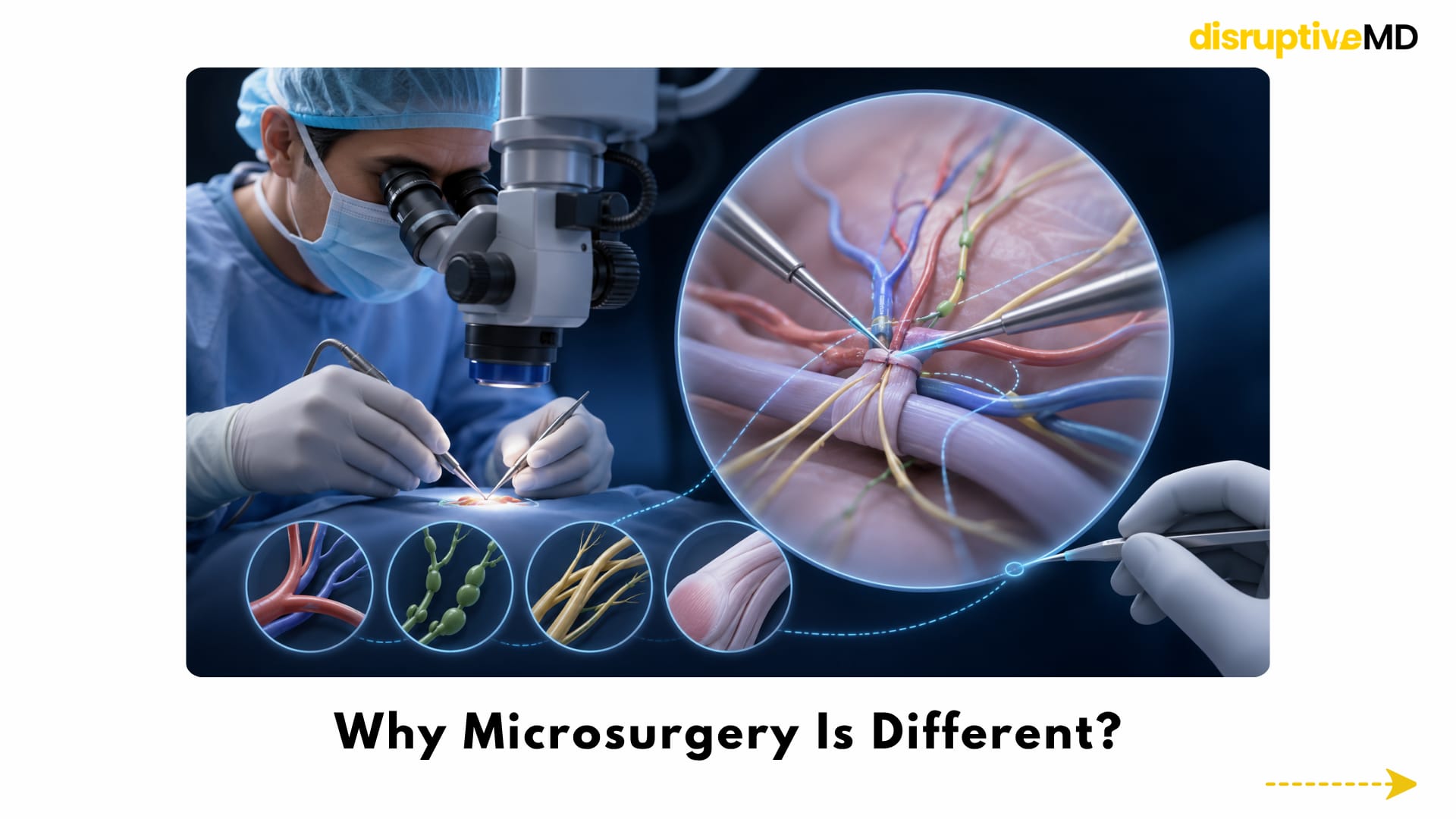
Why Microsurgery Is Different?
Microsurgery is not simply “small surgery.”
It is surgery where the target structures are so delicate that precision directly affects survival, healing, and function.
Microsurgeons may repair or connect:
- small blood vessels
- lymphatic vessels
- peripheral nerves
- tiny tissue flaps
- delicate reconstructive tissues
- ducts or tubular structures
- vascularised grafts
In reconstructive surgery, a tiny blood vessel connection can determine whether a transferred tissue flap survives. In nerve repair, alignment may influence recovery potential. In lymphatic surgery, extremely small lymphatic channels may need to be connected to small veins to improve drainage.
This is why microsurgery requires exceptional hand control, patience, visual focus, and years of training.
Robotic microsurgery enters the field because it supports the exact things that make microsurgery difficult: steadiness, scale, precision, and endurance.
Microsurgery vs Supermicrosurgery
Microsurgery usually deals with small vessels and nerves.
Supermicrosurgery goes even smaller.
It may involve extremely tiny vessels, lymphatic channels, perforators, fingertip structures, or delicate nerve branches. This is especially important in lymphatic surgery, fingertip reconstruction, perforator flaps, nerve repair, and advanced reconstructive procedures.
As the structures become smaller, the margin for error becomes narrower. The needle is smaller.
The suture is finer.
The tissue is more fragile.
The movement must be more controlled.
This is one reason robotic systems are so exciting. They may help surgeons perform movements at a scale where even highly trained human hands reach their natural limits.
Motion Scaling: Turning Large Movements Into Tiny Movements
Motion scaling is one of the most important advantages of robotic microsurgery.
In manual surgery, the surgeon’s hand movement directly moves the instrument.
In robotic microsurgery, that relationship can be changed.
If the surgeon moves their hand several millimetres, the robotic instrument may move only a fraction of that distance. This allows larger, comfortable hand movements to become extremely small, controlled instrument movements.
It is like translating human motion into microsurgical motion.
This can help with needle positioning, suture placement, vessel alignment, tissue manipulation, and delicate dissection.
At microscopic scale, precision is not only about reaching the right place. It is about reaching it gently.
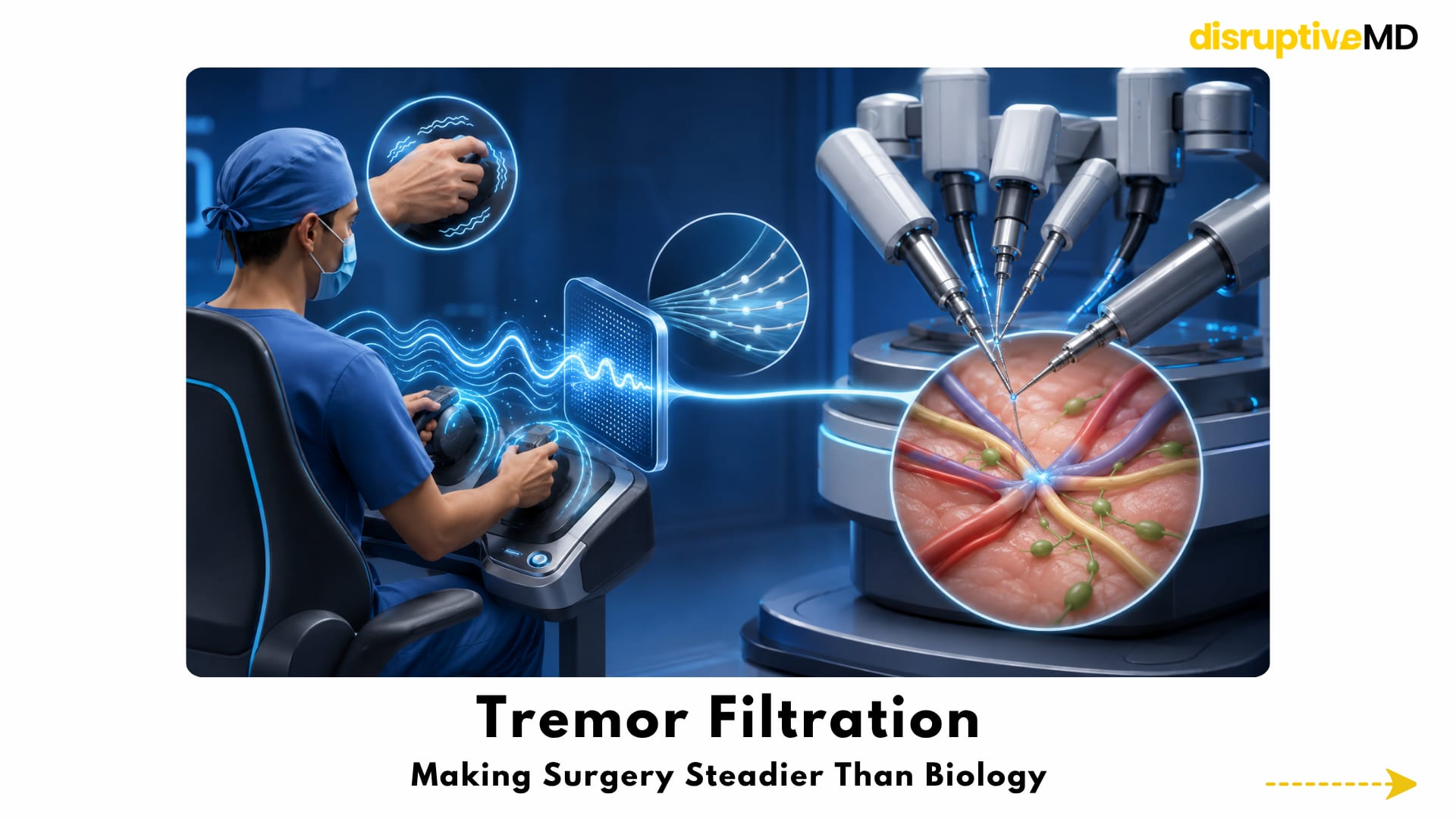
Tremor Filtration: Making Surgery Steadier Than Biology
Every human hand has some natural tremor.
At normal surgical scale, this may not matter much. But when operating on a tiny lymphatic vessel or small blood vessel, even a movement that is barely visible can affect precision.
Robotic systems can filter tremor before it reaches the instrument tip.
This does not mean the robot is operating independently.
It means the surgeon’s intended movement is preserved, while unwanted vibration is reduced.
This may support more stable suturing, more controlled needle handling, more delicate vessel manipulation, and safer tissue positioning in very small surgical fields.
This is one of the most powerful ideas in robotic microsurgery: The surgeon remains in control, but the movement becomes digitally steadier.
Better Ergonomics for Surgeons
Traditional microsurgery often requires long hours in difficult positions under a microscope.
Surgeons may experience neck strain, shoulder fatigue, back discomfort, eye strain, and hand fatigue during complex cases.
Robotic systems may allow surgeons to work from a more ergonomic console or seated position. This could reduce physical strain and help maintain precision during long procedures.
This matters because surgeon fatigue is not just a comfort issue.
Fatigue can affect concentration, steadiness, and performance.
Robotic microsurgery may therefore improve not only technical precision, but also the sustainability of microsurgical careers.
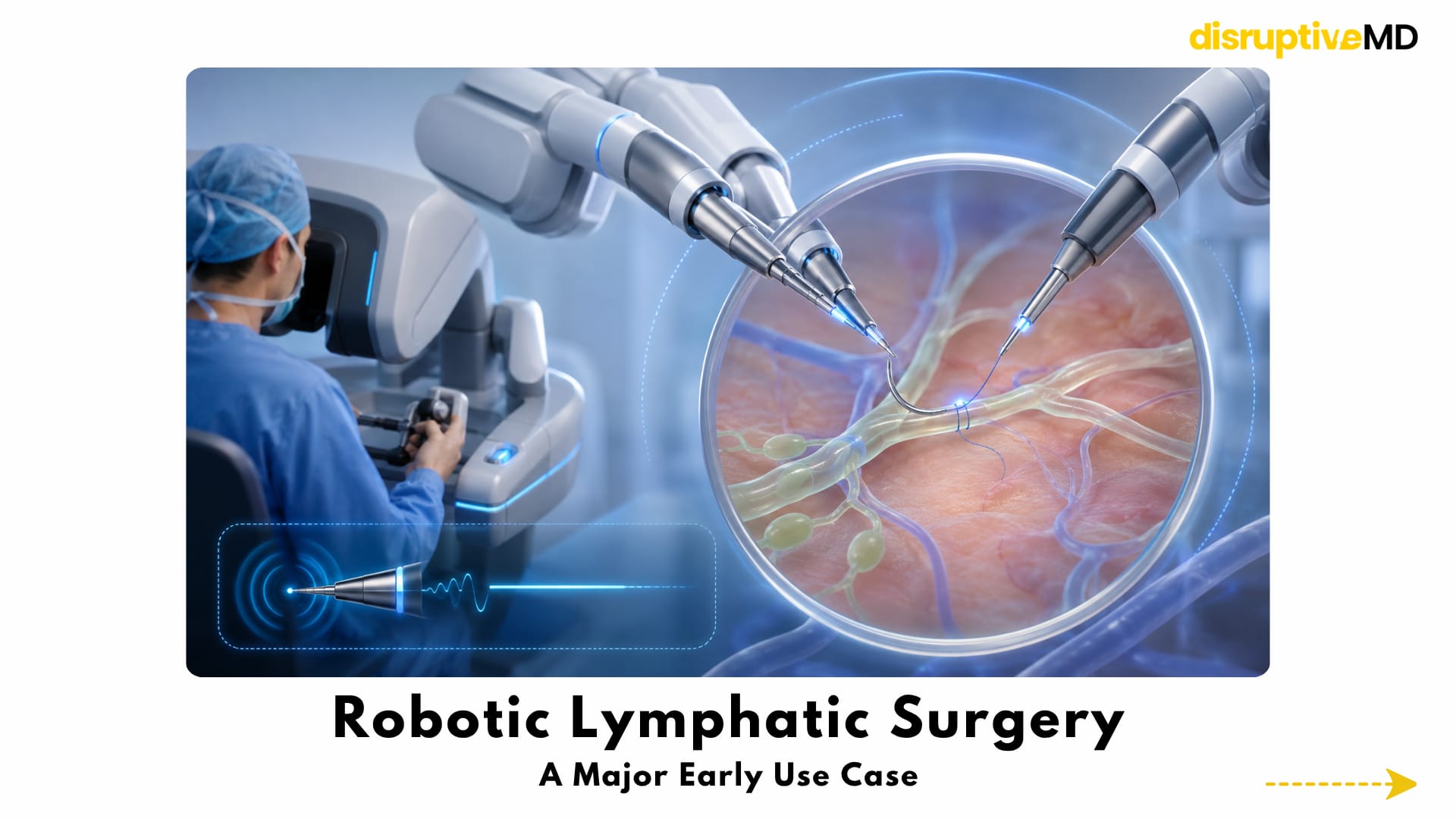
Robotic Lymphatic Surgery: A Major Early Use Case
One of the strongest early applications of robotic microsurgery is lymphatic surgery.
Lymphatic vessels are extremely small, thin, and fragile. They can be difficult to see, handle, and connect.
This matters in lymphedema, a condition where lymph fluid does not drain properly. It can occur after cancer surgery, radiation, trauma, infection, or lymphatic injury. Patients may experience swelling, heaviness, discomfort, recurrent infections, reduced movement, and reduced quality of life.
One advanced surgical option is lymphovenous anastomosis.
This means connecting tiny lymphatic channels to small veins so lymph fluid can bypass blocked pathways.The field is tiny.The vessels are fragile.The movements must be extremely controlled.
Robotic assistance may support tremor reduction, motion scaling, stable needle handling, and precise suturing in lymphatic reconstruction. This is why lymphedema surgery is one of the most important real-world examples of robotic microsurgery.
Blood Vessel Anastomosis and Reconstructive Surgery
Anastomosis means connecting two tubular structures.
In microsurgery, this often means joining tiny blood vessels so that transferred tissue can survive.
This is central to free flap reconstruction, where tissue is moved from one part of the body to another along with its blood supply. These procedures are used in breast reconstruction, head and neck reconstruction, limb reconstruction, trauma reconstruction, facial reconstruction, and complex wound coverage.
Robotic assistance may help improve stability and precision during microvascular suturing.
It may support better control of needle angle, vessel alignment, suture spacing, and tissue handling.
However, this is also where evidence and validation matter.
Expert manual microsurgery is already highly successful in many centres. Robotic microsurgery must prove where it adds real value, especially in very small vessels, deep spaces, long procedures, training, or supermicrosurgery.
The real question now is: When does robotic precision improve outcomes compared with expert human hands?
Nerve Repair and Hand Surgery
Nerve repair is another area where precision matters.
Peripheral nerves are living communication pathways. When they are injured, repair may require careful alignment, gentle handling, nerve grafting, or nerve transfer.
Tiny differences in alignment may influence the pathway available for nerve regeneration.
Robotic microsurgery could eventually support delicate nerve coaptation, peripheral nerve repair, nerve grafting, and reconstructive nerve procedures.
Hand and limb surgery may also benefit because many structures are small but functionally critical. A fingertip vessel, digital nerve, small artery, or tendon-adjacent tissue plane can have a major impact on sensation, movement, and function.
Potential applications include:
- fingertip reconstruction
- digital replantation
- peripheral nerve repair
- small vessel repair
- complex trauma reconstruction
- vascularised bone grafts
- delicate hand and limb reconstruction
In hand surgery, small anatomy can create big consequences. That is exactly where robotic precision may matter.
Ophthalmic, Neurosurgical, and Transplant Possibilities
Some of the most futuristic applications of robotic microsurgery may appear in ophthalmology, neurosurgery, and transplantation.
Eye surgery already requires extraordinary precision. Robotic systems may eventually assist with retinal surgery, subretinal injections, membrane peeling, corneal microsurgery, microcannulation, and microscale drug delivery.
This is especially important as the future of eye care may involve gene therapy, cell therapy, and regenerative treatments that need to be delivered into extremely precise tissue layers.
Neurosurgery and spine surgery also involve tiny, high-risk spaces. Future systems may assist selected procedures involving small vessels, cranial nerves, tumour corridors, spinal microsurgery, microvascular decompression, and skull base surgery.
This area requires extreme caution because the safety threshold is very high.
In transplantation, robotic microsurgery may eventually support tissue transplantation, hand transplantation, face transplantation, composite tissue allotransplantation, and small vessel reconstruction.
The future of transplantation may also involve engineered tissues and regenerative implants. Those tissues will not only need to be created. They will need to be connected.
Robotic Microsurgery and Regenerative Medicine
Regenerative medicine is moving toward engineered tissues, vascularised grafts, nerve guides, biologic scaffolds, organoids, and possibly bioprinted tissues.
But creating tissue is only one part of the challenge.
The tissue must survive inside the body.
It needs blood supply.
It may need nerve integration.
It must connect with surrounding tissue.
This is where robotic microsurgery could become a bridge between regenerative medicine and real clinical use.
If future bioprinted or engineered tissues need tiny vascular connections, robotic microsurgery may help connect them to the patient’s circulation.
This links robotic microsurgery with the future organ factory. The tissue may be made in the lab. But the final connection may happen in the operating room.
Read more on Future of Organ Factory Article
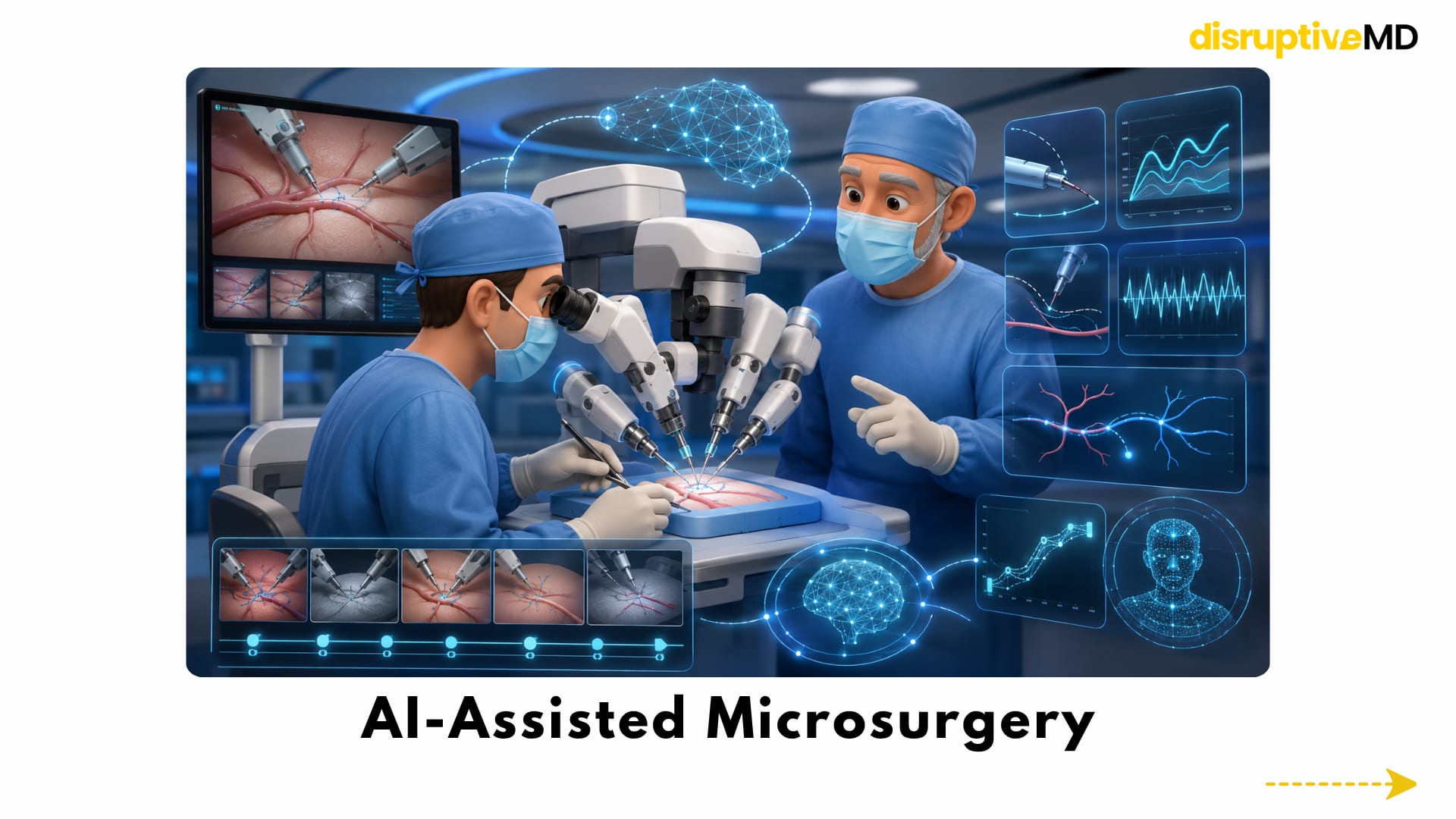
AI-Assisted Microsurgery
The next step is not only robotic control. It is robotic microsurgery combined with AI.
AI may support microsurgery by analysing:
- instrument tracking
- tremor patterns
- motion efficiency
- tissue recognition
- needle angle
- suture spacing
- vessel alignment
- error detection
- performance feedback
- surgical video
- training progress
This could turn microsurgical performance into measurable data.
Instead of relying only on subjective feedback, future systems may show how smooth a movement was, how accurate the suture spacing was, how much tremor occurred, and how a trainee is improving over time.
This could make microsurgical training more structured, objective, and scalable.
The mentor remains essential. But AI can become a performance mirror.
It can help show what the human eye may miss. Read more on Surgery without large incisions Article
From Expert-Only Skill to Wider Access
One of the most disruptive possibilities is access.
Today, advanced microsurgery and supermicrosurgery are often concentrated in specialised centres. These procedures require elite training, specialised equipment, and experienced teams.
If robotic systems make ultra-precise movements more stable and reproducible, some highly specialised procedures may eventually become available in more centres.
The goal is not to make microsurgery easy.
The goal is to make elite precision more scalable.
However, this future is not guaranteed.
Robotic systems are expensive. Training takes time. Operating room workflow must change. Early cases may take longer. Hospitals need infrastructure, maintenance, and trained teams.
So the access question is important: Will robotic microsurgery democratise precision? Or will it remain limited to elite centres? The answer will depend on cost, validation, training, and real-world patient outcomes.
Partial Automation: The Realistic Future
The future of robotic microsurgery is probably not full robot autonomy.
The more realistic future is partial automation.
This means the surgeon remains in control, while the system assists selected delicate steps.
Examples may include:
- needle positioning
- vessel alignment assistance
- tremor-free suture placement
- spacing guidance
- instrument stabilisation
- camera tracking
- motion constraint zones
- force or tension alerts
This is a more believable and safer vision than fully autonomous surgery.
The surgeon provides judgement.
The robot provides precision support.
The future may not be a robot surgeon.
It may be a surgeon with a robotic microsurgical co-pilot.
The Big Limitations
Robotic microsurgery is exciting, but it is not perfect.
One major limitation is haptic feedback.
In manual microsurgery, surgeons can feel tissue resistance, vessel fragility, needle passage, and suture tension. Robotic systems may reduce that sense of touch.
This matters because microsurgical tissues are delicate. Too much force can damage a vessel, tear a lymphatic channel, crush a nerve, or injure fragile tissue.
Future systems will need better force sensing and haptic feedback.
Other limitations include:
- High cost
- Maintenance
- Disposable instruments
- Training requirements
- Operating room setup
- Longer early operative times
- Workflow changes
- Limited availability
- Need for stronger clinical validation
Robotic microsurgery must prove that it improves outcomes, reduces complications, supports training, reduces fatigue, or expands access enough to justify the investment.
Technology alone is not enough. Patient benefit is the real standard.
What Is Possible Today
What is real today:
- Robotic systems can assist selected microsurgical and supermicrosurgical procedures.
- Tremor filtration and motion scaling are major technical advantages.
- Lymphatic surgery is one of the strongest early use cases.
- Robotic assistance may improve ergonomics and precision.
- Training may benefit from objective motion data and simulation.
What is not fully real yet:
- Robots replacing microsurgeons
- Routine autonomous microsurgery
- Perfect haptic feedback
- Affordable access everywhere
- Universal proof of better outcomes across all procedures
- Widespread use in every hospital
- Fully automated vessel or nerve repair in routine care
This distinction is important. Robotic microsurgery is real. But the most futuristic version is still being built.
Fact Base
Microsurgery involves operating on extremely small structures such as blood vessels, lymphatic vessels, nerves, and delicate reconstructive tissues.
Supermicrosurgery goes even smaller, often involving tiny vessels and lymphatic channels that demand extreme precision.
Human hands have natural limits, including tremor, fatigue, posture strain, and limited motion scaling.
Robotic microsurgery can support surgeons through tremor filtration, motion scaling, improved stability, ergonomic control, and precise robotic microinstruments.
Lymphatic surgery is one of the strongest early use cases because lymphatic vessels are extremely small and fragile.
Robotic microsurgery may also support microvascular reconstruction, nerve repair, hand surgery, ophthalmic procedures, transplantation, regenerative medicine, and future bioprinted tissue implantation.
AI may further improve the field by analysing instrument movement, tremor, suture spacing, tissue recognition, training performance, and surgical video.
The main limitations are cost, learning curve, haptic feedback, workflow challenges, operative time, and the need for stronger outcome evidence.
The most realistic future is surgeon-controlled robotic assistance, not full robot replacement.
Future Vision
The future robotic microsurgery platform may combine:
- tremor filtration
- motion scaling
- high-resolution 3D visualisation
- robotic microinstruments
- AI video analysis
- force sensing
- haptic feedback
- digital twin planning
- microsurgical simulation
- automated performance feedback
- remote expert support
- partial automation of selected steps
This could create a new era where human judgement and robotic precision work together.
The surgeon would still decide.
The robot would help execute.
AI would help measure.
Force sensing would help protect tissue.
Simulation would help train the next generation.
Regenerative medicine and bioprinting may provide new tissues.
Robotic microsurgery may help connect them to the living body.
Final Takeaway
Robotic microsurgery is not about replacing the hand of the surgeon.
It is about transforming the surgeon’s hand into a digitally refined instrument capable of working at a scale where even tiny movements matter.
The future of surgery may not only be minimally invasive. It will be microscopically precise.
References
- van Mulken TJM, Schols RM, Scharmga AMJ, et al. First-in-human robotic supermicrosurgery using a dedicated microsurgical robot for treating breast cancer-related lymphedema: a randomized pilot trial.Nature Communications. 2020;11:757. DOI: https://doi.org/10.1038/s41467-019-14188-w
- van Mulken TJM, Wolfs JAGN, Qiu SS, et al. One-Year Outcomes of the First Human Trial on Robot-Assisted Lymphaticovenous Anastomosis for Breast Cancer–Related Lymphedema. Plastic and Reconstructive Surgery.2022;149(1):151–161. DOI: https://doi.org/10.1097/PRS.0000000000008670
- Malzone G, Menichini G, Innocenti M, et al. Microsurgical robotic system enables the performance of microvascular anastomoses: a randomized in vivo preclinical trial. Scientific Reports. 2023;13:14003. DOI: https://doi.org/10.1038/s41598-023-41143-z
- Ghandourah HSH, Schols RM, Wolfs JAGN, Altaweel F, van Mulken TJM. Robotic Microsurgery in Plastic and Reconstructive Surgery: A Literature Review. Surgical Innovation. 2023;30(5):607–614. DOI: https://doi.org/10.1177/15533506231191211
- Kueckelhaus M, Nistor A, van Mulken T, et al. Clinical experience in open robotic-assisted microsurgery: user consensus of the European Federation of Societies for Microsurgery. Journal of Robotic Surgery. 2025;19:171. DOI: https://doi.org/10.1007/s11701-025-02338-w
- Stögner VA, et al. Robotic-Assisted Microsurgery in Lymphatic Reconstruction. Journal of Craniofacial Surgery. 2025;36(1):359–362. DOI: https://doi.org/10.1097/SCS.0000000000010608
- Edwards TL, Xue K, Meenink HCM, et al. First-in-human study of the safety and viability of intraocular robotic surgery. Nature Biomedical Engineering. 2018;2:649–656. DOI: https://doi.org/10.1038/s41551-018-0248-4
- Cehajic-Kapetanovic J, Xue K, Edwards TL, et al. First-in-Human Robot-Assisted Subretinal Drug Delivery Under Local Anesthesia. American Journal of Ophthalmology. 2022;237:104–113. DOI: https://doi.org/10.1016/j.ajo.2021.11.005
- Mi H, MacLaren RE, Cehajic-Kapetanovic J. Robotising vitreoretinal surgeries. Eye. 2025;39:673–682. DOI: https://doi.org/10.1038/s41433-024-03149-3
- Yang K, Jin X, Wang Z, et al. Robot-assisted subretinal injection system: development and preliminary verification. BMC Ophthalmology. 2022;22:484. DOI: https://doi.org/10.1186/s12886-022-02720-4
- Sugiyama T, Tang M, Sugimori H, et al. Artificial intelligence-integrated video analysis of vessel area changes and instrument motion for microsurgical skill assessment. Scientific Reports. 2025;15:27898. DOI: https://doi.org/10.1038/s41598-025-13522-1
- Amirabdollahian F, Livatino S, Vahedi B, et al. Prevalence of haptic feedback in robot-mediated surgery: a systematic review of literature. Journal of Robotic Surgery. 2018;12:11–25. DOI: https://doi.org/10.1007/s11701-017-0763-4
- Selim M, et al. A comprehensive review of haptic feedback in minimally invasive robotic surgery. International Journal of Medical Robotics and Computer Assisted Surgery. 2024. DOI: https://doi.org/10.1002/rcs.2605
- Prasad SM, Maniar HS, Soper NJ, Damiano RJ, Klingensmith ME. Surgical robotics: impact of motion scaling on task performance. Journal of the American College of Surgeons. 2004;199(6):863–868. DOI: https://doi.org/10.1016/j.jamcollsurg.2004.07.002
- Barbash GI, Glied SA. New Technology and Health Care Costs — The Case of Robot-Assisted Surgery. New England Journal of Medicine. 2010;363:701–704. DOI: https://doi.org/10.1056/NEJMp1006602