
What if major surgery no longer required major cuts?
For most of medical history, surgery was defined by exposure.
To reach a diseased organ, damaged joint, bleeding vessel, tumour, fracture, or deep anatomical target, surgeons often had to create large incisions and open the body widely. The incision was the price paid for visibility, access, and control.
But modern surgery is entering a different era.
Today, many procedures can be performed through tiny incisions, ports, scopes, catheters, needles, natural openings, image-guided pathways, robotic instruments, and energy-based tools.
The goal is not simply to make surgery “smaller.”
The real goal is: To reduce tissue trauma while preserving or improving surgical precision, safety, visibility, and recovery.
This is the next era of minimally invasive care. Not just smaller surgery. Smarter access.

- Open surgery remains one of the most important tools in medicine.
- The body does not always need to be widely opened to treat disease.
- Keyhole surgery has changed modern care by separating access from exposure.
From open surgery to keyhole thinking
Open surgery remains one of the most important tools in medicine. It gives direct access, tactile feedback, wide exposure, and rapid control in complex or dangerous situations.
But the old assumption has changed.
The body does not always need to be widely opened to treat disease.
Keyhole surgery changed modern care by separating access from exposure. Instead of a large incision, surgeons can enter through small ports and use cameras, screens, long instruments, scopes, or robotic systems to reach the same internal target.
This shift transformed surgery because the surgeon’s eye no longer had to be directly inside an open wound.
- The camera became the eye.
- The port became the doorway.
- The screen became the surgical field.
- The instrument became an extension of the hand.
The future of surgery may be less about how much anatomy is exposed, and more about how precisely the target can be reached.
Laparoscopy: the abdominal revolution
Laparoscopic surgery is one of the clearest examples of minimally invasive care.
It uses small incisions, a camera, and long instruments to operate inside the abdomen or pelvis. It has changed procedures such as gallbladder surgery, appendix surgery, hernia repair, bariatric surgery, colorectal surgery, gynaecological surgery, urological surgery, and selected abdominal cancer operations.
The major idea is not only that the incisions are smaller.
Laparoscopy creates a magnified internal view and allows surgeons to work with controlled precision through small access points.
But it also demands a different skill set. Surgeons must work through a screen, understand camera-based depth, coordinate long instruments, and manage complications through limited access.
This is an important truth: Minimally invasive surgery is not automatically easier. Sometimes it is more technically demanding.
Arthroscopy: Orthopaedic precision inside the joint
Arthroscopy brought minimally invasive surgery into orthopaedics and sports medicine.
Instead of opening a joint widely, surgeons place a small camera inside the joint and use specialised instruments through tiny portals.
It is widely used in shoulder arthroscopy, knee arthroscopy, meniscus repair, ACL reconstruction, rotator cuff repair, labral repair, hip arthroscopy, and cartilage procedures.
For sports medicine, this is especially important because the goal is not only to repair anatomy. The goal is to preserve function, protect healthy tissue, and support recovery.
Arthroscopy shows how minimally invasive surgery can treat delicate structures while reducing unnecessary disruption to surrounding tissue.
A joint does not always need to be opened widely. Sometimes it needs to be entered intelligently.
Limb endoscopy: Orthopaedic precision outside the joint
Orthopaedic endoscopy represents the next frontier of minimally invasive surgery, extending beyond traditional arthroscopy into the extra-articular spaces where tendons, nerves, fascia, bursae, and soft-tissue planes can be visualized and treated with precision.
While arthroscopy is primarily intra-articular, endoscopy explores the anatomy outside the joint.
This has opened new possibilities in shoulder periscapular and subacromial procedures, elbow distal biceps repairs and reconstructions and ulnar nerve surgery, hand and wrist tendon and nerve endoscopy, hip peritrochanteric and hamstring endoscopy, knee posteromedial and extra-articular ligament procedures, and foot and ankle tendoscopy.
With advances in optics, navigation, biologics, robotics, and augmented reality, orthopaedic endoscopy is evolving from a minimally invasive technique into a precision platform for tissue-preserving surgery.
Endoscopy and endoluminal surgery: using the body’s own pathways
Endoscopic surgery uses flexible or rigid scopes to diagnose and treat disease through small openings or natural body passages.
It is used in gastrointestinal care, ENT, spine surgery, urology, pulmonary medicine, and neurosurgery.
Endoluminal surgery goes one step further. It treats disease from inside hollow organs or vessels.
Examples include endoscopic lesion removal, endovascular aneurysm repair, transcatheter valve procedures, gastrointestinal endoscopic procedures, ureteroscopic stone treatment, and bronchoscopic interventions.
This is a major shift in surgical thinking. The body’s tubes, i.e. blood vessels, airways, digestive tract, and urinary tract are not only anatomy. They are access routes. Instead of cutting down to disease from the outside, doctors can sometimes reach it from the inside.
Interventional radiology: surgery through needles and catheters
Some of the most minimally invasive procedures are performed without traditional surgical exposure.
Interventional radiology uses imaging guidance such as ultrasound, CT, MRI, or fluoroscopy to guide needles, wires, catheters, balloons, coils, stents, drains, and ablation probes.
This allows treatment through tiny punctures rather than large incisions.
It can be used for angioplasty, stenting, embolisation, tumour ablation, biopsy, drainage, varicose vein treatment, uterine fibroid embolisation, spine procedures, vascular access, and emergency bleeding control.
The disruptive idea is powerful: A procedure can be guided by images instead of by opening the body.
- A bleeding vessel may be controlled from inside the vascular system.
- A tumour may be destroyed with an image-guided ablation probe.
- A blocked artery may be opened through a catheter.
- A fluid collection may be drained through a needle path.
This is procedural medicine without the traditional image of surgery.
- No large incision.
- No wide exposure.
- Just a precise route to the target.
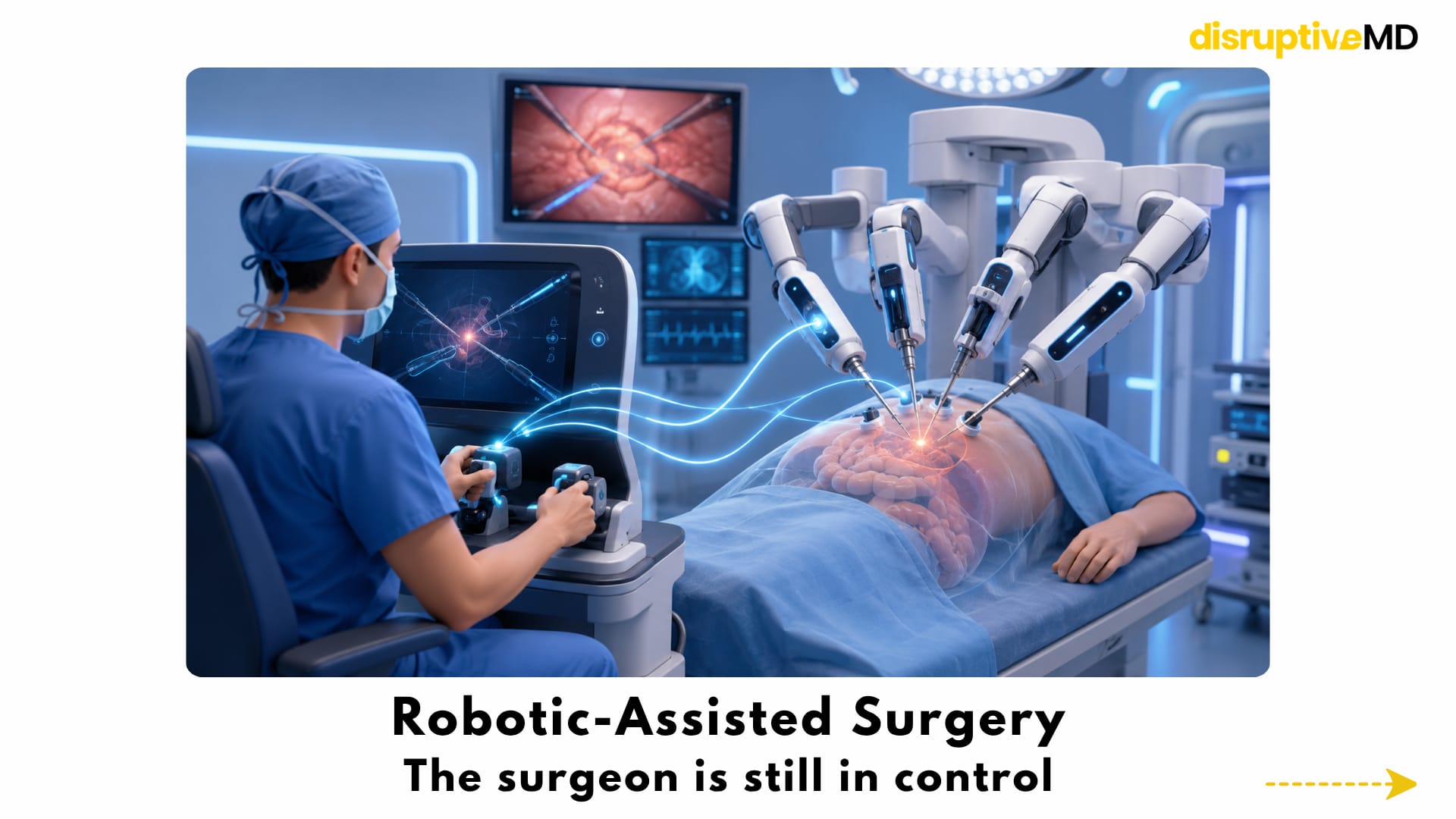
Robotic-assisted surgery: the surgeon is still in control
Robotic surgery does not mean the robot operates alone.
In robotic-assisted surgery, the surgeon controls robotic instruments from a console. The system translates the surgeon’s movements into precise instrument motion inside the patient.
Robotics may offer 3D vision, magnification, tremor filtering, motion scaling, wristed instruments, and improved dexterity in tight spaces.
This matters because straight laparoscopic tools have limits. Human hands are incredibly skilled, but they cannot physically enter deep narrow spaces through tiny ports.
Robotic instruments can bend, rotate, and articulate in ways that may help surgeons operate with greater control in selected procedures.
The disruptive idea is not “robot replaces surgeon.”
The disruptive idea is: Technology expands what the surgeon’s hands can do through a smaller opening.
Read more on : Robotic Surgery Article
Single-port and natural-orifice surgery: fewer visible scars, bigger technical demands
Single-port surgery aims to perform procedures through one small incision instead of multiple ports.
Natural-orifice surgery explores access through existing body openings such as the mouth, vagina, rectum, or urethra.
The futuristic goal is clear:
- Fewer external incisions.
- Less visible scarring.
- Potentially less access trauma.
- A more hidden route into the body.
But these approaches are technically demanding.
Instruments may crowd each other. Angles may be limited. Infection control becomes critical. Closure must be secure. Surgeon training and patient selection are essential.
A smaller entry point is not automatically better if it makes the operation less safe or less effective.
The future of single-port and natural-orifice surgery will depend on better instruments, flexible robotics, advanced imaging, and strong clinical validation.
Image-guided surgery: seeing without exposing
The less anatomy is exposed directly, the more important imaging becomes.
Modern minimally invasive care increasingly depends on ultrasound, fluoroscopy, CT, MRI, intraoperative imaging, navigation systems, 3D reconstruction, and augmented reality overlays.
Image guidance allows surgeons and interventional specialists to locate the target, plan the route, track tools, and avoid critical structures.
This is especially important in spine surgery, neurosurgery, ENT surgery, orthopaedics, tumour surgery, vascular procedures, and image-guided ablation.
Augmented reality and surgical navigation: the operating room becomes a map
Augmented reality and mixed reality may allow surgeons to see digital anatomy overlaid on the real surgical field.
This could include tumour boundaries, blood vessels, nerves, planned surgical paths, implant positions, or danger zones.
Navigation systems can also act like surgical GPS, helping guide instruments toward the target while avoiding vital structures.
This is particularly relevant in spine surgery, neurosurgery, orthopaedics, ENT surgery, tumour surgery, and image-guided ablation.
But surgical AR is not simple.
Organs move. Tissue deforms. Breathing changes anatomy. Blood and instruments alter the view. A digital overlay must be accurate and updated, or it can mislead instead of help.
The future is not just beautiful holograms. The future is reliable surgical guidance.
AI-assisted minimally invasive surgery: the intelligent layer
Minimally invasive surgery produces enormous visual data.
Every laparoscopic, robotic, endoscopic, arthroscopic, and microscopic procedure can generate video. That video contains information about anatomy, instruments, surgical steps, movement, tissue handling, bleeding, workflow, and technical performance.
AI may help analyse this data.
It may support anatomy recognition, instrument tracking, step recognition, surgical video analysis, error detection, workflow optimisation, risk prediction, automated documentation, and training feedback.
The goal is to give the surgeon better information at the right moment.
AI may become the intelligent layer of the minimally invasive operating room: watching the procedure, recognising patterns, supporting decisions, and helping teams learn from surgical video.
But this must be validated carefully.
Surgery is not a controlled laboratory scene. Anatomy varies. Blood, scar tissue, inflammation, obesity, cancer, emergency conditions, and unexpected complications can change everything.
AI in surgery must prove safety and reliability in the real world.
Read more on : AI that watches surgery
Digital twin surgery: testing the operation before entering the body
A digital twin is a virtual model of a patient’s anatomy, disease, or surgical plan.
In the future, digital twins may help surgeons test different approaches before the operation begins.
They could support patient-specific anatomy mapping, access-route planning, implant selection, tumour planning, risk prediction, surgical rehearsal, and personalised strategy.
This connects minimally invasive surgery with precision medicine.
Instead of asking, “What is the standard route?” The surgeon may ask: What is the safest route for this patient?
Digital twins could make surgery more customised, more predictable, and more rehearsed before the first incision is made.
The procedure may become smaller on the outside because the planning becomes deeper on the inside.
Read more on : Digital twin surgery article
Energy-based surgery and ablation: destroying disease without removing large tissue blocks
Modern minimally invasive procedures often depend on energy.
Energy devices include electrosurgery, radiofrequency ablation, laser, ultrasonic tools, microwave ablation, cryoablation, plasma-based devices, and focused ultrasound.
These tools can cut, seal, shrink, destroy, or treat tissue through small access points.
Ablation is especially important because some tumours or abnormal tissues can be destroyed using heat, cold, microwave, radiofrequency, laser, or focused ultrasound instead of being surgically removed through a large incision.
This is central to interventional oncology.
The future may include more treatments where disease is targeted and destroyed without open surgical removal. But ablation requires careful selection. Doctors must consider tumour type, size, location, nearby structures, imaging visibility, margins, recurrence risk, and long-term outcomes.
The question is not only: Can we destroy it? The better question is: Can we destroy it safely, completely, and meaningfully for the patient?
Focused ultrasound: surgery without a traditional incision
Focused ultrasound is one of the most futuristic areas of procedural medicine.
It uses concentrated sound energy to target tissue deep inside the body. In selected conditions, it may allow treatment without a traditional incision.
The concept is extraordinary.
- Energy enters from outside the body.
- Imaging guides the target.
- The treatment effect happens deep inside.
- No conventional cut may be required.
Focused ultrasound represents one of the most extreme forms of minimally invasive or non-invasive procedural care. It requires precise targeting, imaging guidance, safety monitoring, patient selection, and evidence for each specific condition.
Its future is exciting because it asks a radical question: What if some operations could become image-guided energy treatments?
Smart instruments, haptics, and force sensing
One limitation of minimally invasive and robotic surgery is reduced touch.
In open surgery, surgeons can feel tissue tension, resistance, stiffness, pressure, fragility, and danger.
In laparoscopic and robotic surgery, that tactile feedback may be reduced.
Future systems may use force sensing, tactile feedback, and haptic technology to help surgeons understand what instruments are feeling inside the body.
This could help with tissue tension, grip force, suture pressure, traction, resistance, and the risk of tearing delicate structures.
The next generation of instruments may also include miniaturised cameras, steerable catheters, flexible robotic arms, smart needles, tissue-sensing probes, sensor-equipped tools, and capsule-based devices.
The instrument of the future may not simply be a tool. It may be a sensor, camera, navigator, energy device, and data generator at the same time.
Faster recovery is the promise, not the guarantee
The patient-centered promise of minimally invasive surgery is powerful.
In many procedures, smaller access can reduce tissue trauma, scarring, pain, blood loss, wound problems, hospital stay, and recovery time.
It can also support same-day discharge, early mobilisation, faster rehabilitation, home monitoring, telemedicine follow-up, and quicker return to work or sport.
But this should not be overstated.
Minimally invasive surgery is not automatically better for every patient, every disease, or every surgeon.
A small incision does not always mean a small operation inside the body.
The right approach depends on anatomy, disease severity, surgeon expertise, equipment, cost, safety, emergency risk, and expected outcome.
The best operation is not always the smallest one.
The best operation is the one that achieves the goal safely and effectively for that patient.
Where minimally invasive care is reshaping specialties
Minimally invasive surgery is not one specialty. It is changing many fields at once.
In spine surgery, tubular retractors, endoscopy, navigation, robotics, and smaller muscle-sparing approaches are changing decompression, discectomy, fusion, and screw placement.
In cancer surgery, minimally invasive care must balance smaller incisions with oncological safety, margins, lymph node assessment, tumour handling, reconstruction, and long-term outcomes.
In orthopaedic surgery, arthroscopy, percutaneous fracture fixation, minimally invasive plate osteosynthesis, robotic joint replacement, navigation-guided alignment, and sports surgery are reducing unnecessary tissue disruption.
In neurosurgery, endoscopic skull base surgery, keyhole brain surgery, stereotactic biopsy, laser ablation, navigation-guided tumour surgery, and minimally invasive spine surgery are creating smaller corridors to delicate targets.
In cardiac care, catheter-based procedures such as angioplasty, stents, transcatheter valve procedures, structural heart repair, electrophysiology ablation, and left atrial appendage closure show how some conditions can be approached through blood vessels rather than large openings.
This is the larger pattern: The future of surgery is becoming more targeted, more image-guided, more digital, and more personalised.
The new operating room
The minimally invasive operating room of the future may combine robotics, AI, endoscopy, intraoperative imaging, navigation, 3D displays, augmented reality, digital twins, smart instruments, sensor data, and surgical video analytics.
This turns the OR into a connected precision environment.
The surgeon may not rely on one screen or one tool.
Instead, the surgical team may work with multiple layers of information: anatomy, imaging, instrument position, surgical phase, patient physiology, tissue feedback, risk alerts, and video analysis.
The OR begins to look less like a traditional operating room and more like an intelligent cockpit.
The surgeon remains the pilot. Technology becomes the navigation system.
Training, cost, and access
Minimally invasive surgery has a learning curve.
Surgeons must learn camera-based depth perception, hand-eye coordination, instrument triangulation, robotic console control, image-guided anatomy, endoscopic orientation, complication management, and when to convert to open surgery.
This means training must evolve.
Simulation, robotic training, surgical video review, AI-based feedback, virtual reality, mentoring, and objective skill assessment may become essential.
Cost is another major issue.
Robots, imaging systems, navigation platforms, disposable instruments, software, maintenance, and training can be expensive.
The critical question is: Will the next era of minimally invasive surgery reach everyone, or only elite hospitals?
A technology is not truly disruptive if it is impressive but inaccessible.
The future must be advanced, safe, validated, and scalable.
When open surgery is still better
The future is not “open surgery is outdated.”
Open surgery remains essential.
It may still be preferred in major trauma, complex anatomy, severe adhesions, uncontrolled bleeding, large tumours, advanced disease, emergencies, and cases where minimally invasive access compromises safety.
This is one of the most important points in the article.
A small incision is not a guarantee of better care.
A safe operation is better care.
The future is not open surgery versus minimally invasive surgery. The future is choosing the right access for the right patient.
Fact Base
Minimally invasive care is a broad family of techniques that reduce access trauma while using cameras, scopes, catheters, imaging, robotics, navigation, energy devices, and digital planning.
Laparoscopy, arthroscopy, endoscopy, interventional radiology, endoluminal therapy, robotic-assisted surgery, and catheter-based procedures all represent different forms of minimally invasive care.
Robotic-assisted surgery is surgeon-controlled. The robot does not independently operate in routine clinical practice. Image guidance, navigation, and augmented reality are becoming more important because less direct exposure requires better spatial information.
AI may help analyse surgical video, recognise anatomy, track instruments, identify surgical steps, support workflow, and improve training — but real-world validation remains essential.
Digital twins may help create patient-specific surgical models for planning, rehearsal, risk prediction, and personalised strategy.
Focused ultrasound represents a highly futuristic direction because selected treatments may be performed using concentrated energy without a traditional incision.
Minimally invasive surgery may reduce pain, scarring, tissue trauma, hospital stay, and recovery time in many procedures, but it is not automatically better for every patient or condition.
Open surgery remains essential in trauma, severe bleeding, complex anatomy, large tumours, advanced disease, emergencies, and situations where safety requires wider exposure.
The best surgical approach is not the smallest approach. It is the safest, most effective, and most appropriate approach for the individual patient.
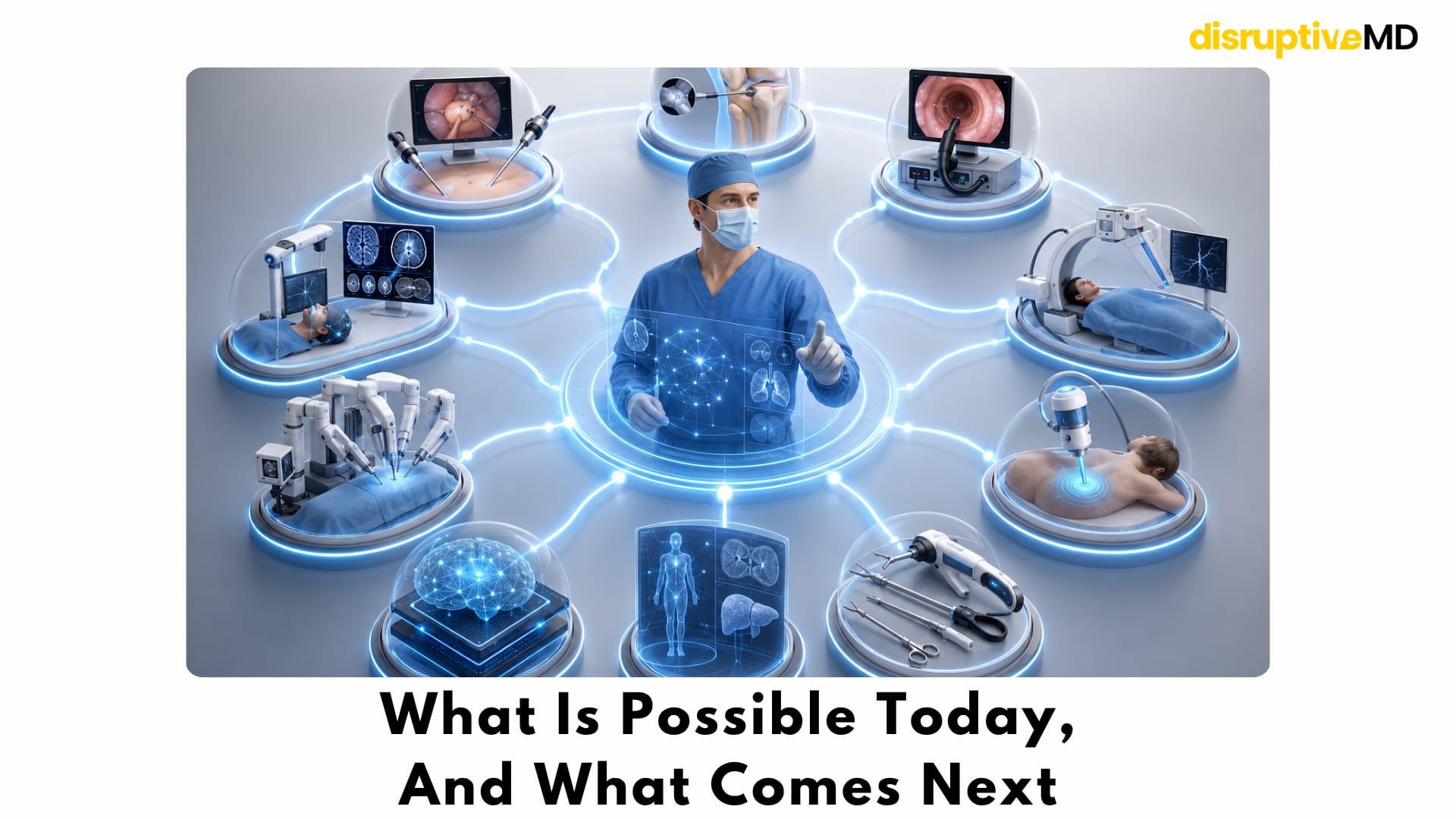
What Is Possible Today, And What Comes Next
Many forms of minimally invasive surgery are already part of routine clinical practice.
Laparoscopic surgery, arthroscopy, endoscopy, interventional radiology, catheter-based cardiac procedures, robotic-assisted surgery, image-guided navigation, and advanced energy devices are already transforming patient care across multiple specialties.
These technologies have changed how surgeons access the body while helping reduce unnecessary tissue disruption in appropriately selected patients.
At the same time, the next generation of minimally invasive care is rapidly evolving.
Artificial intelligence for real-time surgical assistance, digital twin surgical planning, advanced augmented reality guidance, improved haptic feedback, highly flexible robotic systems, smart tissue-sensing instruments, and incisionless therapies such as focused ultrasound are progressing through active research, clinical development, and early adoption in selected settings.
The future is unlikely to be defined by a single breakthrough.
Instead, it will come from combining imaging, robotics, AI, navigation, digital planning, and intelligent instruments into one connected surgical ecosystem.
As these technologies mature, the focus will remain the same:
Deliver safer, more precise, and more personalised surgery while minimising unnecessary tissue trauma.
The future of minimally invasive surgery is not about making the incision smaller.
It is about making every decision smarter.
Final takeaway
Major surgery does not always have to mean major cuts.
But the future is not about chasing the smallest incision at any cost.
It is about choosing the smartest, safest, and most precise path into the body.
The next era of surgery may be measured not by how much we open the body, but by how intelligently we enter it.
References
- Jeganathan JR, Jegasothy R, Sia WT. Minimally invasive surgery: a historical and legal perspective on technological transformation. Journal of Robotic Surgery. 2025. DOI: https://doi.org/10.1007/s11701-025-02589-7
- Mashoufi R, Mashoufi R. Interventional Radiology for Disease Management: A Narrative Review. Cureus. 2023. DOI: https://doi.org/10.7759/cureus.48603
- Campbell WA, Chick JFB, Shin DS, Makary MS. Value of interventional radiology and their contributions to modern medical systems. Frontiers in Radiology. 2024. DOI: https://doi.org/10.3389/fradi.2024.1403761
- Cepolina F, Razzoli R. Review of robotic surgery platforms and end effectors. Journal of Robotic Surgery. 2024. DOI: https://doi.org/10.1007/s11701-023-01781-x
- Paracchini S, Taliento C, Pellecchia G, et al. Artificial intelligence in the operating room: A systematic review of AI models for surgical phase, instruments and anatomical structure identification. Acta Obstetricia et Gynecologica Scandinavica. 2025. DOI: https://doi.org/10.1111/aogs.70045
- Asciak L, Kyeremeh J, Luo X, et al. Digital twin assisted surgery, concept, opportunities, and challenges. npj Digital Medicine. 2025. DOI: https://doi.org/10.1038/s41746-024-01413-0
- Mekki YM, Luijten G, Hagert E, et al. Digital twins for the era of personalized surgery. npj Digital Medicine. 2025. DOI: https://doi.org/10.1038/s41746-025-01575-5
- Izadifar Z, Izadifar Z, Chapman D, Babyn P. An Introduction to High Intensity Focused Ultrasound: Systematic Review on Principles, Devices, and Clinical Applications. Journal of Clinical Medicine. 2020. DOI: https://doi.org/10.3390/jcm9020460
- Bhatia DN, Malviya P. All-endoscopic approach for distal biceps tendon pathology: analysis of long-term outcomes in partial and complete ruptures. J Shoulder Elbow Surg. 2024 Jul;33(7):1601-1614. doi: 10.1016/j.jse.2024.01.020. Epub 2024 Feb 27.
- Bernasconi A, Sadile F, Smeraglia F, Mehdi N, Laborde J, Lintz F. Tendoscopy of Achilles, peroneal and tibialis posterior tendons: An evidence-based update. Foot Ankle Surg. 2018 Oct;24(5):374-382. doi: 10.1016/j.fas.2017.06.004. Epub 2017 Jun 21.
- Nabi Z, Reddy DN. Natural orifice transluminal endoscopic surgery: history and current development. Clinical Endoscopy. 2026. DOI: https://doi.org/10.5946/ce.2025.009
- Pearl JP, Ponsky JL. Natural Orifice Translumenal Endoscopic Surgery: A Critical Review. Journal of Gastrointestinal Surgery. 2008. DOI: https://doi.org/10.1007/s11605-007-0424-4
- Bergholz M, Ferle M, Weber BK, et al. The benefits of haptic feedback in robot assisted surgery and their moderators: a meta-analysis. Scientific Reports. 2023. DOI: https://doi.org/10.1038/s41598-023-46641-8
- Meulstee JW, et al. Augmented Reality Implementation in Minimally Invasive Surgery of Deformable Organs: A Systematic Review. Surgical Innovation. 2024. DOI: https://doi.org/10.1177/15533506241290412