
Introduction
For most of surgical history, planning an operation has depended on a powerful combination of imaging, anatomy, experience, judgement, and technical skill. A surgeon looks at scans, studies the patient’s condition, anticipates possible risks, and mentally builds a plan before entering the operating room. That process is already highly sophisticated, but it still has one major limitation: the real test happens on the real patient.
Digital twin surgery asks a different question.
What if the surgical team could first operate on a virtual version of the patient?
A digital twin is not simply a 3D picture. It is a patient-specific virtual model of a real organ, tumour, joint, blood vessel, spine, heart, or surgical pathway. It can be built from medical imaging, clinical data, biomechanics, artificial intelligence, surgical data, and sometimes real-time sensor information. In its most advanced form, it does not only show anatomy. It predicts behaviour.
This is what makes the idea so disruptive. Surgery is no longer moving only toward smaller cuts, better cameras, or more precise robots. It is moving toward prediction. The future operating room may not begin with the first incision. It may begin with a simulation.
From Seeing Anatomy to Predicting Behaviour
A 3D anatomical model can help a surgeon understand shape. It can show the location of a tumour, the curve of a bone, the branching of blood vessels, or the size of an implant. This is already useful, especially in complex cases where standard imaging is difficult to mentally reconstruct.
A digital twin goes further.
It may simulate how tissues move, how blood flows, how pressure changes, how a joint carries load, how an implant behaves, how a tumour relates to nearby structures, or how the body may respond after surgery. This difference matters because the most difficult surgical decisions are rarely only about what something looks like. They are about what will happen when the surgeon acts.
- If a vessel is clamped, how will circulation change?
- If a tumour is removed, what tissue must be preserved?
- If a spine is corrected, how will alignment and load distribution shift?
- If an implant is placed, will it fit, move, loosen, or wear over time?
- If a robotic instrument follows one path instead of another, will it avoid critical structures?
- A 3D model answers, “What is there?”
- A digital twin tries to answer, “What may happen next?”




- A digital twin is a patient-specific virtual model of a real organ, tumour, joint, blood vessel, spine, heart, or surgical pathway.
- It can be built from medical imaging, clinical data, biomechanics, artificial intelligence, surgical data, and sometimes real-time sensor information.
- In its most advanced form, it does not only show anatomy. It predicts behaviour.
Testing the Operation Before the Operation
The most powerful idea in digital twin surgery is surgical rehearsal. Before performing a high-risk operation, the team could test different surgical strategies inside a virtual version of the patient.
In tumour surgery, this could mean comparing different resection pathways to remove cancer while protecting blood vessels, nerves, ducts, or functional tissue. In vascular surgery, it could mean simulating how blood flow may change after a repair, graft, stent, or bypass. In spine surgery, it could mean testing alignment correction before placing screws or rods. In joint reconstruction, it could mean comparing implant sizes, angles, and movement patterns before opening the patient.
This is not about replacing clinical judgement. It is about giving clinical judgement a new environment to work inside.
The surgeon is still the decision-maker. The digital twin becomes a rehearsal space, a risk map, and a prediction engine. Instead of asking the surgeon to rely only on mental simulation, the system allows the team to test the plan visually, mechanically, and physiologically.
Patient-Specific Anatomy Matters
Textbook anatomy is useful, but patients do not arrive in textbook form.
One patient may have unusual blood vessel branching. Another may have scar tissue from previous surgery. A tumour may distort nearby structures. A congenital abnormality may change the entire surgical route. A spine deformity, pelvic injury, joint malalignment, or complex fracture may make standard planning less reliable.
Digital twins could help surgery move from population anatomy to individual anatomy. Instead of planning around an average patient, the team could plan around this patient, this organ, this tumour, this joint, and this risk profile.
That shift is central to precision medicine.
Precision surgery is not only about doing a procedure accurately. It is about choosing the right procedure, the right route, the right implant, the right margin, the right reconstruction, and the right recovery plan for the individual patient.
Digital Twins in Cardiac Surgery and Cardiology
The heart is one of the most exciting areas for digital twin development because it is both a structure and a moving biological system. It has anatomy, rhythm, valves, electrical conduction, blood flow, pressure, muscle contraction, and response to devices.
A cardiac digital twin could help clinicians simulate heart rhythm, pumping function, valve behaviour, congenital heart anatomy, blood flow through vessels, or response to interventions. This could be useful in planning ablation procedures for arrhythmias, valve interventions, congenital repairs, device placement, or complex vascular procedures.
For example, in rhythm disorders, a digital version of the patient’s heart could help identify where abnormal electrical circuits may arise and how different ablation strategies may affect them. In valve disease, a twin could help test implant size, position, pressure changes, and flow patterns before the procedure. In congenital heart surgery, where anatomy can be highly individual, a digital twin could help the team understand the safest route through a very unusual structure.
The heart shows why digital twin surgery is more than visualisation. A heart model that only looks like a heart is helpful. A heart model that behaves like the patient’s heart is far more powerful.
Digital Twins in Neurosurgery
In neurosurgery, millimetres matter. The brain and spine contain critical structures where small errors can have major consequences. Tumours, blood vessels, nerves, white matter tracts, spinal cord pathways, and functional brain regions may be tightly packed into very small spaces.
Patient-specific digital models can help surgeons understand the relationship between a lesion and the structures around it. In brain tumour surgery, this may include tumour borders, blood vessels, important functional areas, and fibre tracts involved in movement, speech, vision, or cognition. In spine surgery, it may include the spinal cord, nerve roots, bone anatomy, deformity, tumour involvement, and planned screw or implant trajectories.
When combined with augmented reality, mixed reality, and surgical navigation, digital twins could eventually help surgeons see hidden anatomy overlaid onto the operative field. The surgeon would not only look at a separate screen. The surgical plan could become part of the visual environment.
The future version is even more ambitious: a digital model that updates as the operation progresses. Brain shift, tissue movement, bleeding, swelling, and changes in anatomy can make preoperative images less accurate during surgery. A true intraoperative twin would need to adapt to those changes, not simply display yesterday’s scan.
Digital Twins in Orthopaedics
Orthopaedics is a natural fit for digital twins because bones, joints, implants, alignment, forces, and movement can be modelled mechanically. A hip, knee, shoulder, ankle, spine, or fracture is not only an anatomical structure. It is also a load-bearing system.
In joint replacement, digital twins could help select implant size, position, alignment, and movement mechanics. In spine surgery, they could simulate deformity correction, spinal balance, screw trajectories, and load transfer. In fracture fixation, they could help test plate position, screw placement, stability, and healing conditions. In sports injury reconstruction, they could model ligament tension, joint stability, graft behaviour, and return-to-movement demands.
This could also change postoperative care. A patient-specific twin could combine surgical data with wearable data, gait analysis, rehabilitation progress, pain scores, strength testing, and implant performance. Instead of recovery being judged only by clinic visits and patient reports, the care team could track how the repaired system behaves in the real world.
For sports medicine and rehabilitation, this is especially interesting. Surgery is not the finish line. Return to movement is the true endpoint. A digital twin could help connect the operation to the rehabilitation plan.
Digital Twins in Cancer Surgery
Cancer surgery is not only about removing a tumour. It is about removing enough tumour while preserving enough normal tissue.
That balance is difficult in organs such as the brain, liver, pancreas, lung, pelvis, kidney, and head and neck region. Tumours may wrap around vessels, distort anatomy, invade tissue planes, or move with breathing. Surgeons must think about margins, reconstruction, blood supply, function, and the patient’s ability to recover.
A cancer surgery digital twin could help map tumour boundaries, vascular supply, organ movement, surgical margins, reconstruction options, and functional risk. In liver surgery, it could help estimate how much healthy liver will remain after resection. In brain surgery, it could help protect functional pathways. In pelvic surgery, it could help understand the relationship between tumour, nerves, vessels, and organs. In head-and-neck surgery, it could support reconstruction planning after tumour removal.
The goal is not simply to make cancer surgery more technical. The goal is to make it more personalised, safer, and more deliberate.
Digital Twins and Robotic Surgery
Robotic surgery already gives surgeons better instrument control, tremor filtration, high-definition vision, and access through smaller incisions. But robotic precision does not automatically mean predictive intelligence.
Digital twins may add that missing layer.
In the future, a robotic surgery system could be linked to a patient-specific simulation that shows safe zones, danger zones, tissue tension, blood vessels, tumour margins, and ideal instrument pathways. The robot would still be controlled by the surgeon, but the surgical environment could become more aware.
This could create a new relationship between surgeon, robot, and patient data. The robot provides precision. The digital twin provides prediction. The surgeon provides judgement.
Augmented Reality and Mixed Reality Surgery
One of the most visually exciting possibilities is the projection of the digital twin into the surgeon’s field of view.
Augmented reality and mixed reality could allow surgeons to see virtual anatomy overlaid onto the real patient. Hidden blood vessels, tumour boundaries, planned cutting lines, implant positions, or nerve pathways could appear as navigational guidance during the procedure.
This sounds futuristic, but the technical challenge is serious. The overlay must be accurate. It must move with the patient. It must account for tissue deformation. It must avoid delay. It must not distract the surgeon. In surgery, a beautiful overlay is not enough. It must be trustworthy.
That is why digital twin surgery is not just a design problem. It is a validation problem.
Real-Time Updating: The True Futuristic Layer
A preoperative model is helpful, but the most advanced version of digital twin surgery would update during the operation.
As tissue moves, blood flow changes, instruments interact, imaging updates, or the surgical plan shifts, the digital twin would adjust. It would become a living model of the operation rather than a static plan created before it.
This is extremely difficult. Human tissue is soft, deformable, wet, vascular, and unpredictable. Organs move with breathing and heartbeat. Tumours may not behave exactly like the model predicted. Bleeding can change the field. In minimally invasive surgery, the camera view may show only a small part of the anatomy.
A real-time surgical twin must solve one of the hardest problems in medicine: keeping the virtual patient aligned with the real patient while the real patient is changing.
If that can be done safely, the operating room changes completely. The surgeon would not only perform surgery. The surgeon would operate inside a continuously updated prediction system.
AI-Powered Surgical Prediction
Artificial intelligence can help build and interpret digital twins by analysing medical imaging, surgical videos, electronic health records, biomechanics, sensor information, and outcome data.
AI could help predict surgical difficulty, bleeding risk, complication risk, implant fit, tumour resection feasibility, functional recovery, and the best surgical approach. It could also help identify patterns that are difficult for humans to detect across thousands of cases.
But AI does not make a model automatically correct. A prediction is only useful if it is validated, explainable enough for clinical use, and appropriate for the patient in front of the surgeon. In high-risk surgery, a confident wrong prediction may be more dangerous than no prediction at all.
The future of AI in digital twin surgery should therefore be assistance, not authority.
In Silico Surgery
“In silico” means testing something on a computer. In digital twin surgery, this could mean running virtual surgical scenarios before performing them in real life.
This idea creates a new clinical question:
Before we operate on the patient, should we first operate on the patient’s digital twin?
The answer will depend on the procedure, the quality of the model, the available evidence, and the risk of the operation. For routine surgery, a full digital twin may not be necessary. For complex, rare, high-risk, or anatomically unusual cases, the value may be much higher.
The greatest promise may be in operations where the cost of being wrong is high: brain tumours, congenital heart surgery, aortic aneurysm repair, liver tumour surgery, complex spine deformity, pelvic tumour surgery, revision joint replacement, craniofacial reconstruction, and major trauma reconstruction.
In these cases, even small improvements in planning may matter.
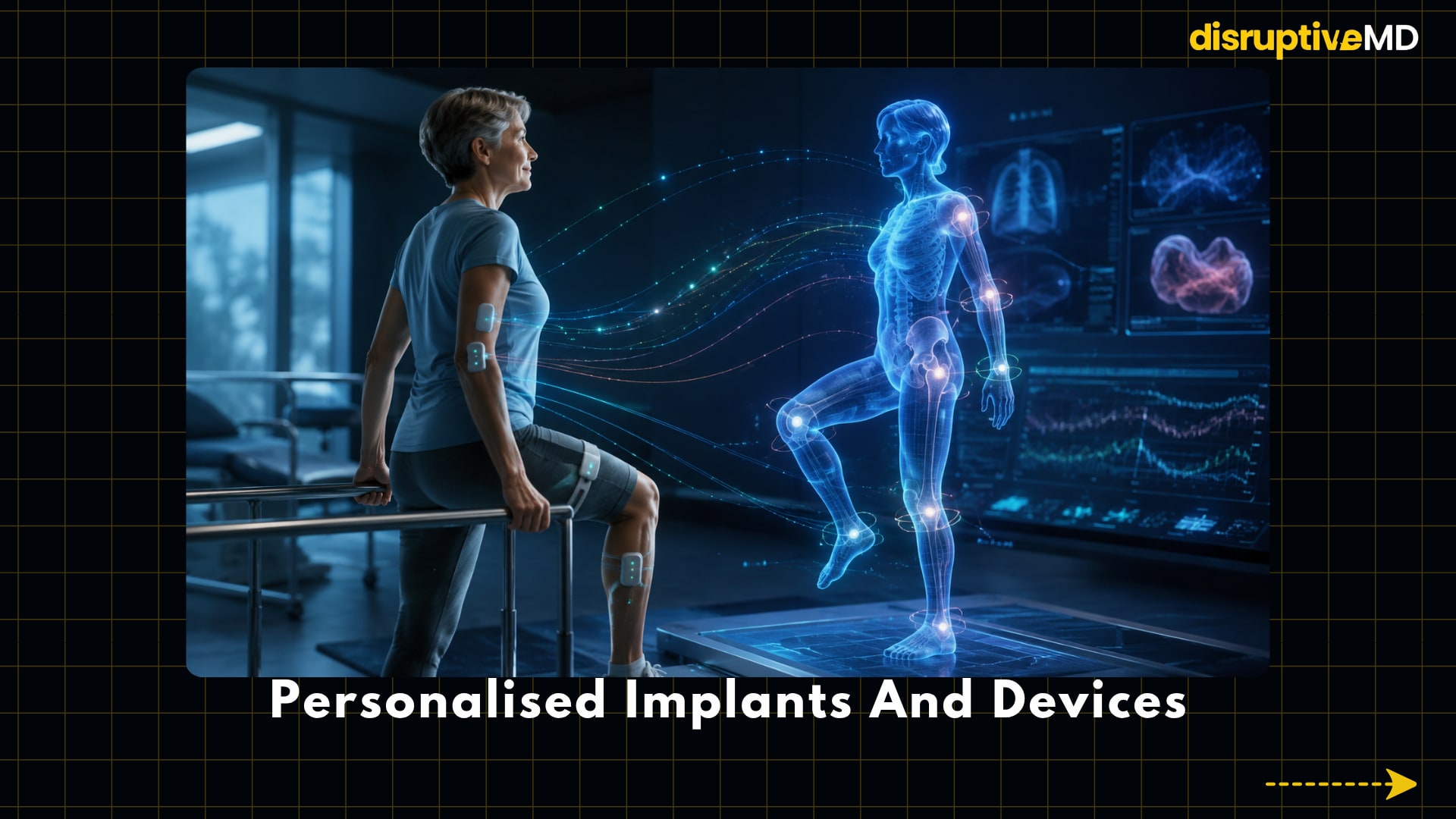
Personalised Implants and Devices
Digital twins could also change the design of implants and surgical devices.
Instead of adapting the patient to standard hardware, surgeons may increasingly adapt hardware to the patient. Patient-specific implants, plates, cutting guides, stents, valves, grafts, prosthetics, and reconstruction devices could be designed using the individual patient’s anatomy and predicted biomechanics.
This is especially relevant in orthopaedics, craniofacial surgery, spine surgery, vascular surgery, and reconstructive surgery. A digital twin could test whether an implant fits, how it distributes force, how it may affect movement, and where failure risk may appear over time.
The future implant may not simply be manufactured for the average body. It may be designed for one body.
Surgical Training on Real Patient Anatomy
Traditional surgical training uses textbooks, cadavers, simulators, videos, and supervised operating room experience. These remain essential, but they do not always prepare a trainee for the exact anatomy of tomorrow’s patient.
Digital twins could allow trainees to rehearse a real case before surgery. A resident could practise a complex fracture fixation, a rare deformity correction, a tumour approach, or a high-risk reconstruction using the patient’s actual anatomy.
This could make surgical training more case-specific and safer. It could also help experienced surgeons prepare for unusual or rare anatomy. Even expert surgeons encounter cases that are outside the routine pattern. A digital twin gives the whole team a way to enter the case before entering the operating room.
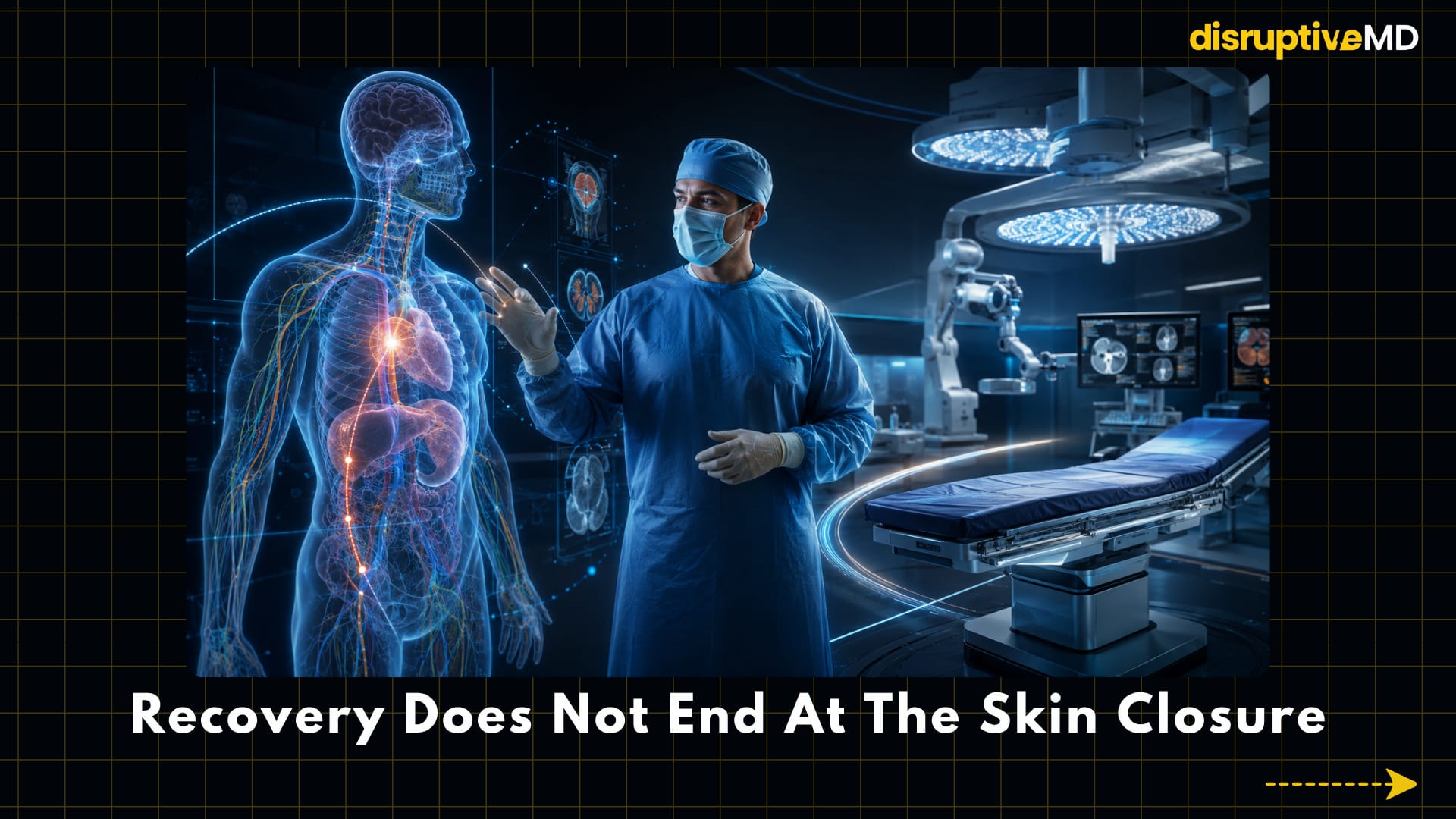
Recovery Does Not End at the Skin Closure
Digital twin surgery should not stop when the operation ends.
Postoperative digital twins could combine wearable data, imaging, movement analysis, wound monitoring, rehabilitation progress, and clinical outcomes to guide recovery. This could be especially useful in orthopaedics, sports medicine, spine surgery, cardiac surgery, and major cancer surgery.
A patient recovering from knee reconstruction may generate movement and gait data. A patient after cardiac surgery may generate heart rate, rhythm, oxygen saturation, sleep, and activity data. A patient after spine surgery may generate mobility and pain trends. A patient after cancer surgery may need monitoring of nutrition, strength, wound healing, and return to function.
A digital twin could help turn this data into a personalised recovery map.
The goal would not be to overwhelm clinicians with more numbers. The goal would be to identify meaningful recovery patterns: who is progressing well, who is at risk of delayed recovery, who may need rehabilitation changes, and who may need earlier review.
Digital Twin Surgery and Precision Rehabilitation
Rehabilitation is often treated as a separate phase after surgery, but in reality, it is part of the treatment.
For orthopaedics, sports medicine, spine surgery, cardiac surgery, and major reconstructive procedures, the operation creates the possibility of recovery, but rehabilitation determines how much function the patient regains.
A digital twin could personalise rehabilitation by modelling strength, mobility, gait, cardiovascular response, tissue healing, implant loading, and return-to-activity progression. Instead of giving every patient the same broad timeline, clinicians could adjust rehabilitation based on the patient’s actual recovery behaviour.
This may be especially valuable for athletes, elderly patients, complex trauma patients, and people recovering from major surgery. The question would shift from “How long since surgery?” to “How is this patient’s body actually adapting?”
Wearables and Continuous Monitoring
Wearables could become one of the major data streams that keep postoperative digital twins updated. Heart rate, activity level, sleep, gait, oxygen saturation, movement quality, and recovery trends may help clinicians understand how the patient is doing outside the hospital.
This matters because most recovery does not happen in the clinic. It happens at home, during sleep, during walking, during rehabilitation, and during normal daily life.
A digital twin connected to real-world monitoring could help detect recovery problems earlier. But there is an important caution: more data does not automatically mean better care. Wearable data must be accurate, clinically meaningful, and interpreted in context. A patient is not a dashboard.
Digital Twin Operating Rooms
The digital twin concept may also extend beyond the patient.
A future hospital could create a digital twin of the operating room itself. This model could simulate workflow, staff movement, equipment placement, robotic positioning, instrument use, infection-control pathways, emergency scenarios, and surgical scheduling.
This could help hospitals improve safety and efficiency before problems occur in real life. For example, a digital twin operating room could test whether a robotic system is positioned safely, whether emergency access is blocked, whether staff movement increases contamination risk, or whether a complex procedure requires a different room layout.
In this version, the “patient twin” helps personalise the operation, while the “OR twin” helps optimise the environment around the operation.
Fact Base
Digital twin surgery is built on several converging technologies: high-resolution medical imaging, 3D reconstruction, computational modelling, biomechanics, artificial intelligence, augmented reality, robotic systems, wearable sensors, and clinical data platforms.
The most important distinction is that a true digital twin should be personalised, dynamically updated, predictive, and useful for decision-making. Many tools called “digital twins” today are advanced 3D models, static simulations, or digital shadows. They may still be useful, but they are not always full digital twins.
Current surgical applications are most advanced in planning, simulation, education, selected cardiac modelling, orthopaedic biomechanics, augmented reality guidance, device testing, and early postoperative monitoring concepts. However, widespread real-time digital twin surgery remains early.
Computational modelling and simulation are increasingly recognised by regulators and researchers as important tools, especially for medical devices and in silico testing. But credibility matters. A model used for clinical decisions must be verified, validated, and tested for uncertainty.
The biggest scientific challenge is not creating a beautiful model. It is proving that the model is accurate enough to improve real patient outcomes.
The Evidence Gap
Digital twin surgery is promising, but it is not yet routine standard practice across most surgical fields.
Many systems are still experimental, early clinical, or limited to specialised centres. Some tools improve visualisation and planning confidence, but the harder question is whether they reduce complications, improve function, shorten recovery, increase survival, lower costs, or improve long-term outcomes.
That difference is important. A digital twin can look impressive and still fail clinically if it does not improve decisions.
For digital twin surgery to become mainstream, it must move beyond “This helps us see better” toward “This helps patients do better.”
Key Challenges
The first challenge is accuracy. A digital twin is only as good as the data and assumptions behind it. Poor imaging, incomplete clinical data, wrong tissue properties, biased training data, or outdated information can make the simulation unreliable.
The second challenge is real-time updating. Surgery changes anatomy. Tissue moves, bleeds, stretches, swells, and deforms. Keeping a virtual model aligned with a changing surgical field is technically difficult.
The third challenge is validation. Digital twins must be tested against real outcomes. It is not enough for the model to appear logical. It must be proven useful within a specific clinical context.
The fourth challenge is surgeon trust. A system that is too opaque, too slow, too distracting, or too difficult to use will not survive in the operating room. Surgical tools must fit into surgical workflow.
The fifth challenge is access. Advanced imaging, computing, sensors, robotics, and mixed reality systems may be expensive. If digital twin surgery becomes available only in wealthy hospitals, it could widen healthcare inequality.
The sixth challenge is responsibility. If a simulation recommends a plan and the plan fails, who is accountable? The surgeon, the hospital, the software developer, the device company, or the data provider?
These questions must be solved before digital twin surgery can become a trusted part of everyday care.
The Most Important Limitation
A digital twin is not the patient.
It is a model of the patient.
That difference must never be forgotten. Models simplify reality. They depend on assumptions. They may miss biological complexity. They may not capture rare anatomy, unexpected bleeding, tissue fragility, inflammation, scarring, surgical judgement, or the unpredictable behaviour of living systems.
A digital twin can support a surgeon, but it cannot replace surgical expertise. It can inform a decision, but it should not own the decision. It can reduce uncertainty, but it cannot eliminate uncertainty.
False confidence may be the greatest danger.
Ethical Questions
Digital twin surgery raises important ethical questions.
- Who owns the patient’s digital twin?
- Can it be used for training?
- Can it be used to test devices?
- Can it be shared between hospitals?
- How long should it be stored?
- Who protects the data?
- Who is responsible if the simulation is wrong?
- Will patients understand when a plan is based partly on prediction?
- Will this technology improve access, or will it create another divide between advanced centres and under-resourced hospitals?
These questions are not side issues. They are central to whether digital twin surgery becomes a trusted medical tool or just another impressive technology with uneven benefits.
Future Vision: The Operating Room Before the Operating Room
The future operating room may combine patient-specific digital twins, AI-assisted surgical planning, robotic surgery, augmented reality overlays, intraoperative imaging, real-time risk prediction, personalised implants, wearable monitoring, and precision rehabilitation.
A patient with a complex tumour may have a digital twin built before surgery. The team could test different approaches, predict risk to nearby structures, plan reconstruction, and prepare for complications. During surgery, augmented reality could help visualise hidden anatomy. A robotic system could assist with precise movements. Intraoperative imaging could update the model. After surgery, wearables and rehabilitation data could update the twin again, guiding recovery.
This is the real promise: a continuous surgical intelligence system that begins before the incision and continues after discharge.
Final Takeaway
Digital twin surgery is not about replacing surgeons with software.
It is about giving surgeons a virtual patient before the real operation — a space where they can test decisions, understand risk, personalise the plan, and make surgery more precise.
The most powerful message is simple:
The future of surgery may begin before the first incision.
Refrences
-
Mekki YM, Luijten G, Hagert E, et al. Digital twins for the era of personalized surgery. npj Digital Medicine. 2025;8:283. DOI: 10.1038/s41746-025-01575-5 Link: https://doi.org/10.1038/s41746-025-01575-5
-
Asciak L, Kyeremeh J, Luo X, et al. Digital twin assisted surgery, concept, opportunities, and challenges. npj Digital Medicine. 2025;8:32. DOI: 10.1038/s41746-024-01413-0 Link: https://doi.org/10.1038/s41746-024-01413-0
-
Tudor BH, Shargo R, Gray GM, et al. A scoping review of human digital twins in healthcare applications and usage patterns. npj Digital Medicine. 2025;8:587. DOI: 10.1038/s41746-025-01910-w Link: https://doi.org/10.1038/s41746-025-01910-w
-
Katsoulakis E, Wang Q, Wu H, et al. Digital twins for health: a scoping review. npj Digital Medicine. 2024;7:77. DOI: 10.1038/s41746-024-01073-0 Link: https://doi.org/10.1038/s41746-024-01073-0.
-
Dean MC, Oeding JF, Diniz P, Seil R, Samuelsson K, ESSKA Artificial Intelligence Working Group.Leveraging digital twins for improved orthopaedic evaluation and treatment. Journal of Experimental Orthopaedics. 2024;11:e70084. DOI: 10.1002/jeo2.70084 Link: https://doi.org/10.1002/jeo2.70084
-
Ragnhildstveit A, Li C, Zimmerman MH, et al. Intra-operative applications of augmented reality in glioma surgery: a systematic review. Frontiers in Surgery. 2023;10:1245851. DOI: 10.3389/fsurg.2023.1245851 Link: https://doi.org/10.3389/fsurg.2023.1245851
-
National Academies of Sciences, Engineering, and Medicine. Foundational Research Gaps and Future Directions for Digital Twins. Washington, DC: The National Academies Press; 2024. DOI: 10.17226/26894 Link: https://doi.org/10.17226/26894
-
U.S. Food and Drug Administration. Assessing the Credibility of Computational Modeling and Simulation in Medical Device Submissions: Guidance for Industry and Food and Drug Administration Staff. November 2023. Link: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/assessing-credibility-computational-modeling-and-simulation-medical-device-submissions.
-
European Society of Cardiology. Digital twin technology helps reduce the recurrence of atrial arrhythmias after catheter ablation for persistent atrial fibrillation. ESC Press Release. 31 August 2025. Link: https://www.escardio.org/news/press/press-releases/Digital-twin-technology-helps-reduce-the-recurrence-of-atrial-arrhythmias-after-catheter-ablation-for-persistent-atrial-fibrillation/