
From Finding Organs to Building Biology
For most of modern medicine, organ replacement has depended on a difficult reality: the body can fail faster than medicine can replace it.
A kidney may fail.
A liver may lose function.
A heart may weaken.
Skin may be destroyed by burns.
Cartilage may wear down.
Bone may be lost after trauma, tumour surgery, or infection.
Tendons and ligaments may tear and heal poorly.
When tissue is damaged beyond its natural repair capacity, medicine usually turns to a few options: donor organs, grafts, synthetic implants, reconstructive surgery, or long-term disease management.
Each option has limits. Donor organs are scarce. Implants are not living tissue. Grafts may not match perfectly. Some tissues do not regenerate well. And many patients are left waiting for biology to do something it cannot always do.
This is why 3D bioprinting feels so futuristic. It asks a completely different question. Can we manufacture a living replacement?
3D bioprinting is the process of printing living cells, biomaterials, growth factors, and structural scaffolds layer by layer to create tissue-like structures. The dream is not simply to print something that looks like an organ. The goal is to create living tissue that can survive, integrate with the body, and perform a useful biological role.
This distinction matters.
A plastic model of a heart can be printed today.
A metal implant can be 3D printed today.
A surgical guide can be custom-made today.
But printing a living, breathing, vascularised, immune-compatible, mechanically functional organ is a completely different challenge.
This is the future organ factory: a possible future where patient imaging, stem cells, bioinks, artificial intelligence, digital twins, bioreactors, tissue testing, and surgery come together to build personalised living repair systems.
However, bioprinting is not yet a routine solution for printing full transplantable hearts, kidneys, lungs, or livers.
The first revolution may not be printed organs. It may be printed tissues.




- The body can fail faster than medicine can replace it.
- When tissue is damaged beyond its natural repair capacity, medicine usually turns to donor organs, grafts, synthetic implants, reconstructive surgery, or long-term disease management.
- The real goal is to create living tissue that can survive, integrate with the body, and perform a useful biological role.
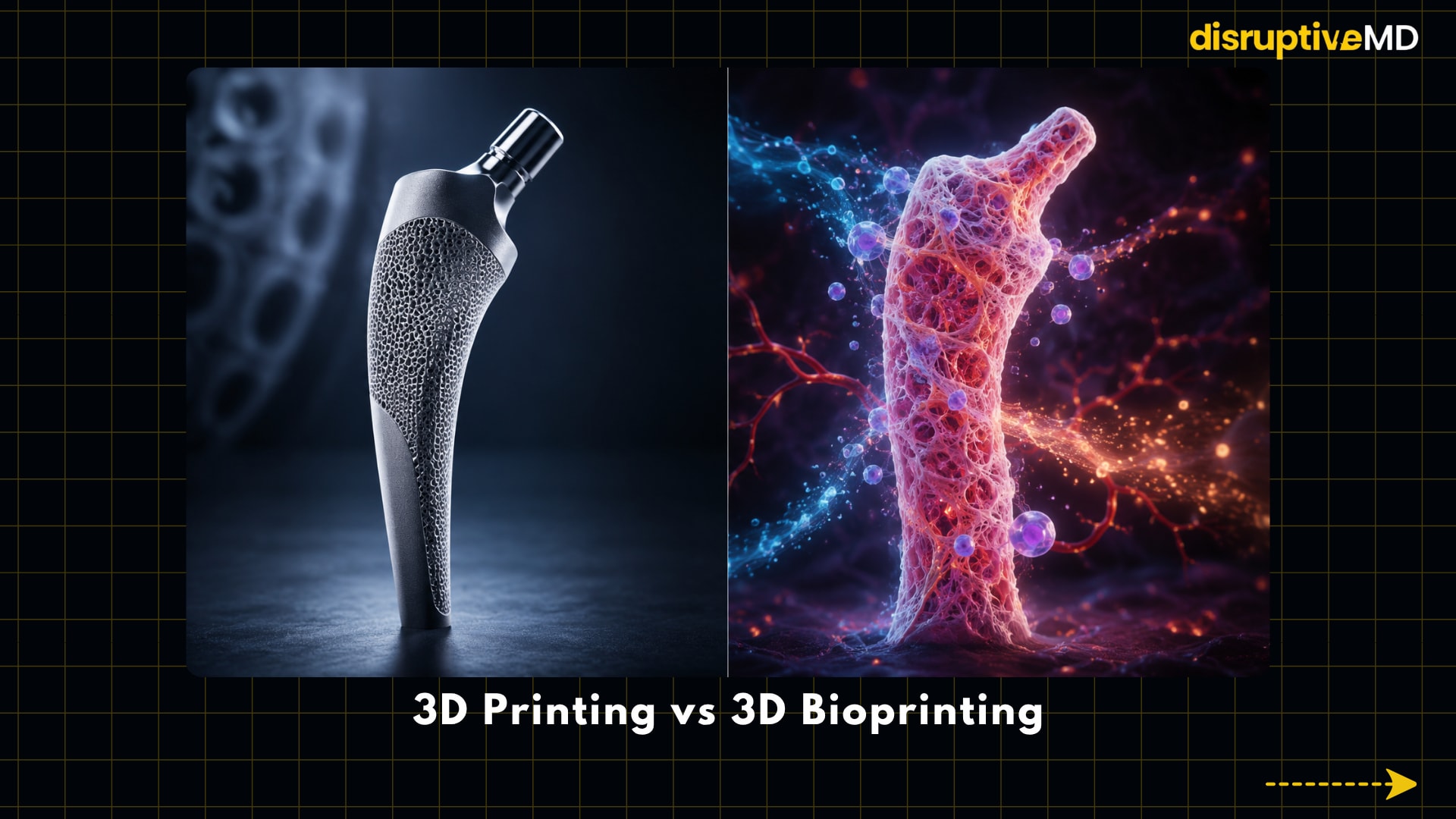
3D Printing vs 3D Bioprinting
3D printing and 3D bioprinting sound similar, but they are not the same.
3D printing usually uses materials such as plastic, metal, ceramic, resin, or polymer. In medicine, this can be used to make surgical guides, anatomical models, dental devices, prosthetics, and some implants. The goal is usually shape, fit, strength, accuracy, and mechanical function.
3D bioprinting is different. It uses living cells and biologically compatible materials. These materials may include hydrogels, extracellular matrix components, growth factors, nutrients, and structural biomaterials that support living cells.
A printed implant needs to fit. A bioprinted tissue needs to live.
It must survive the printing process.
It must receive oxygen and nutrients.
It must remove waste.
It must maintain the right cell behaviour.
It must mature after printing.
It must integrate with the patient’s body.
It must not trigger harmful immune reactions.
It must not grow abnormally.
It must function safely over time.
This is why printing a tissue is not just a manufacturing challenge. It is a biological challenge.
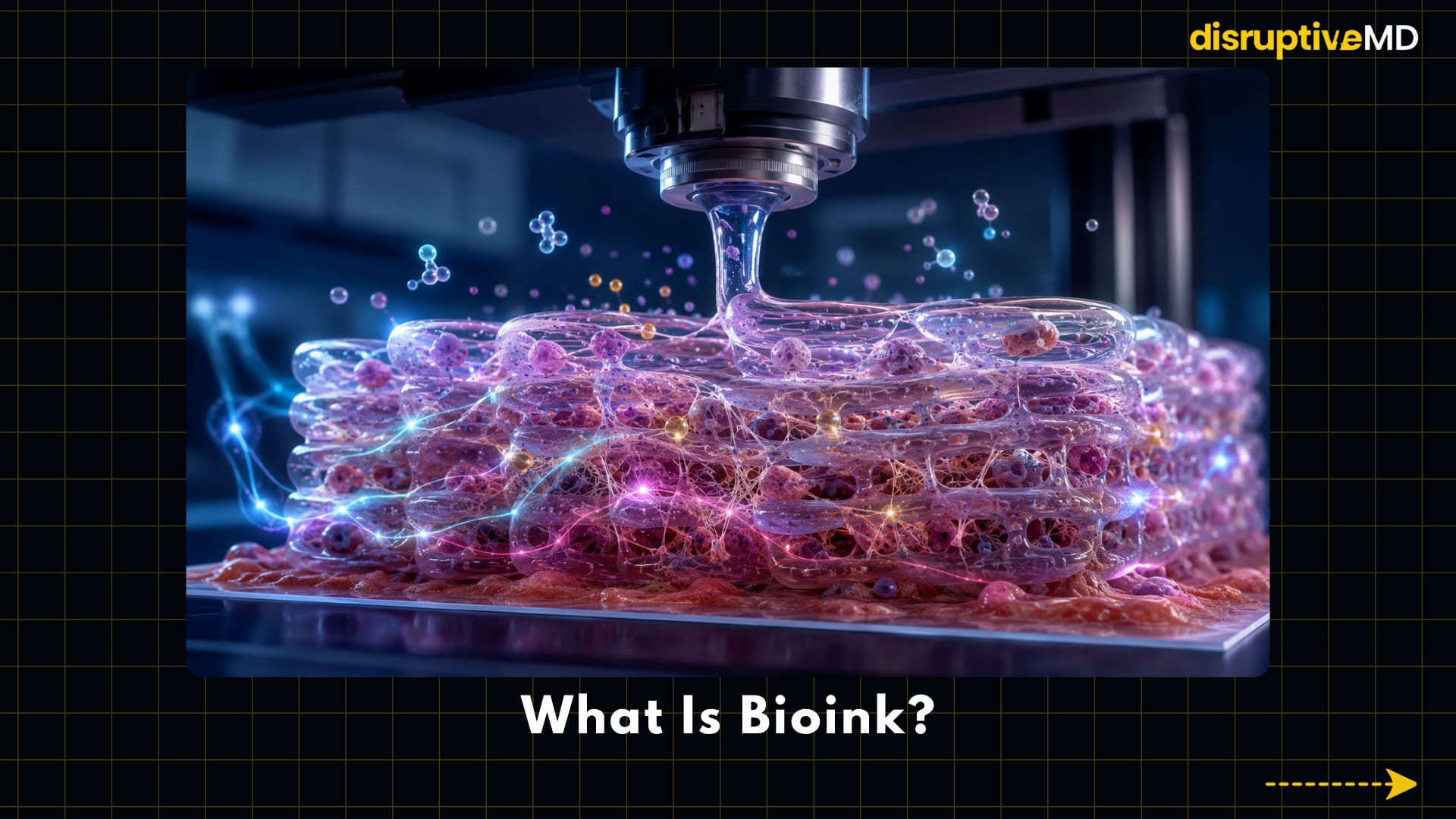
What Is Bioink?
Bioink is the printable biological material used in 3D bioprinting. It is not ordinary ink. It is a living or biologically active material designed to support cells before, during, and after printing.
A bioink may contain: living cells, hydrogels, collagen-like materials, extracellular matrix components, growth factors, nutrients, structural biomaterials, and signalling molecules.
The ideal bioink must do several jobs at once.
-
It must be printable enough to pass through a bioprinter.
-
It must be gentle enough to protect living cells.
-
It must be stable enough to hold shape.
-
It must be biologically active enough to support cell survival.
-
It must provide mechanical strength.
-
It must allow nutrients and oxygen to move through the tissue.
-
It must be safe enough for possible clinical use.
This balance is extremely difficult.
-
If the material is too soft, the printed structure may collapse.
-
If it is too stiff, cells may not behave normally.
-
If printing pressure is too high, cells may be damaged.
-
If the gel does not support cell attachment, the tissue may fail.
-
If it does not degrade or remodel correctly, the body may not integrate it.
Bioink is one of the most important frontiers in bioprinting because it decides whether printing is just shape-making or true tissue engineering.
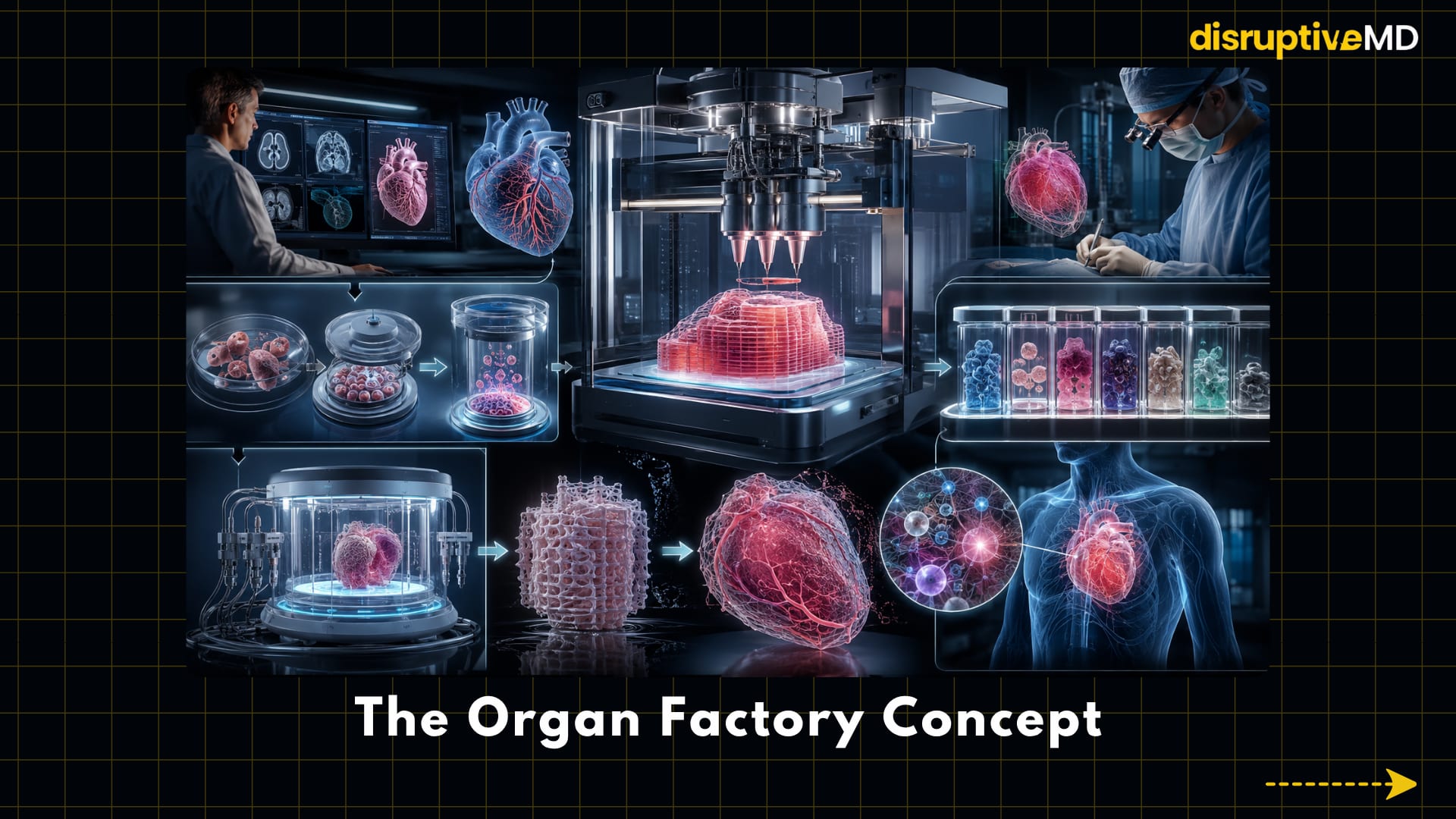
The Organ Factory Concept
The most futuristic vision is the hospital-based biofabrication unit.
Imagine a patient has a complex cartilage defect, a burn wound, a jaw defect, or a piece of heart tissue damaged after disease.
In the future, the workflow could look like this:
-
A patient scan captures the defect.
-
Software converts the scan into a patient-specific design.
-
Cells are collected, expanded, or derived from stem-cell technology.
-
Bioink is selected for the target tissue.
-
A printer builds the living structure layer by layer.
-
A bioreactor matures the tissue under controlled conditions.
-
Quality-control testing checks safety and function.
-
A surgeon implants the tissue.
-
Sensors and imaging monitor healing over time.
This is the organ factory vision. It is not a factory in the ordinary sense. It is a biological manufacturing system. The product is not a machine part. The product is living tissue.
That makes the idea both powerful and complicated. Every printed tissue may need to be personalised, tested, matured, and monitored. The future organ factory would have to combine regenerative medicine, robotics, imaging, artificial intelligence, digital simulation, surgical planning, and strict biological quality control.
The goal is not mass-producing identical organs. The goal is manufacturing repair systems designed for one patient at a time.
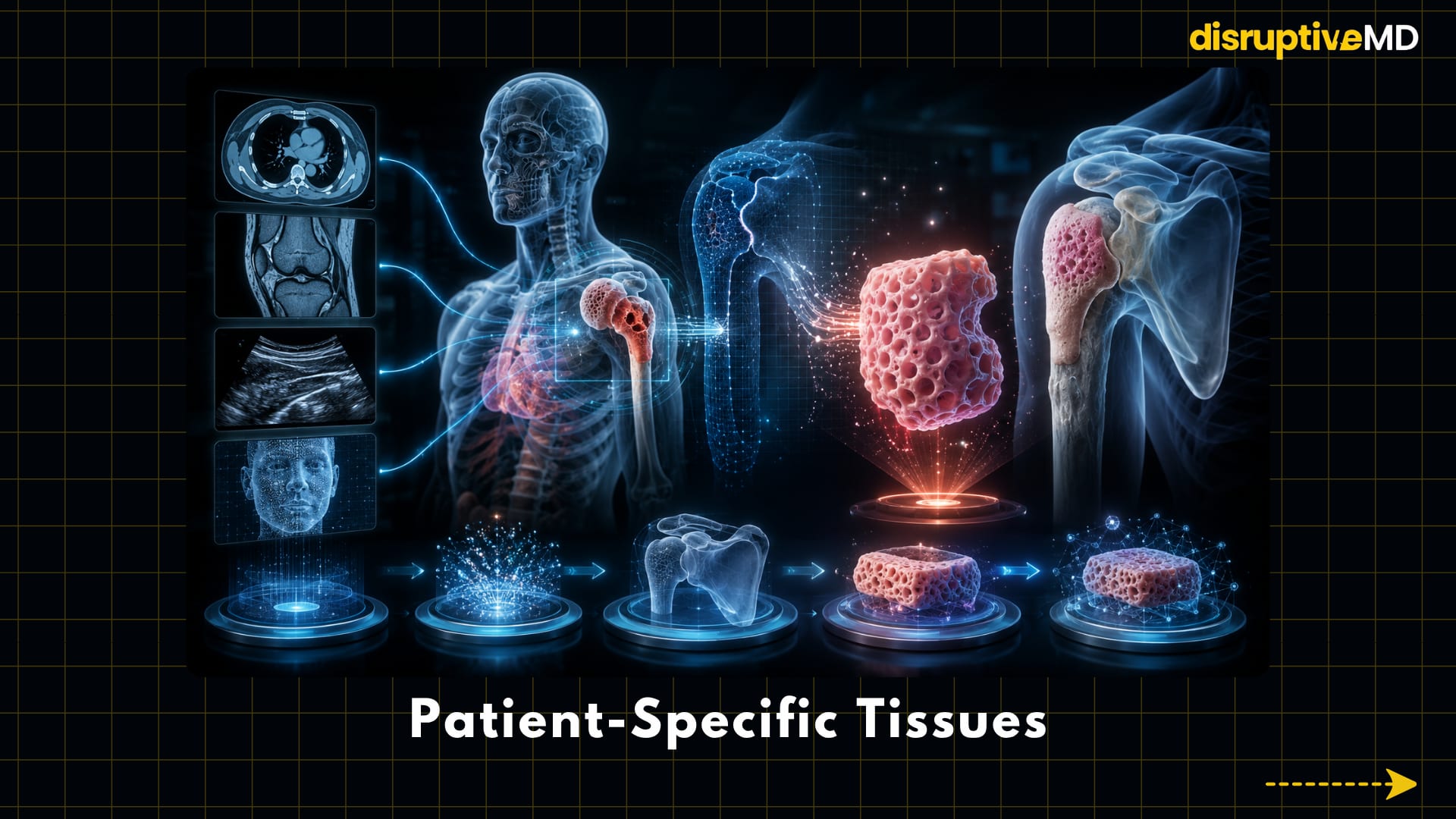
Patient-Specific Tissues
One of the most exciting parts of bioprinting is personalisation.
The body is not built in standard sizes. Bone defects, cartilage injuries, burns, facial defects, vascular injuries, and congenital deformities all have unique shapes.
3D bioprinting could use CT, MRI, ultrasound, or 3D surface scans to design tissues shaped for an individual patient.
This could be especially important for cartilage defects, bone defects burns, facial reconstruction, ear reconstruction, jaw reconstruction, tendon repair, vascular grafts, organ patches, and congenital deformities.
- A patient-specific tissue would not only match the visible shape. Ideally, it would also match the biological environment.
- A cartilage construct would need smoothness and load-bearing ability.
- A bone scaffold would need strength and vascular ingrowth.
- A skin construct would need layered structure.
- A tendon scaffold would need fibre alignment.
- A vascular graft would need flow compatibility.
- A heart patch would need electrical and mechanical coordination.
This is why bioprinting is not just about printing anatomy. It is about printing function.
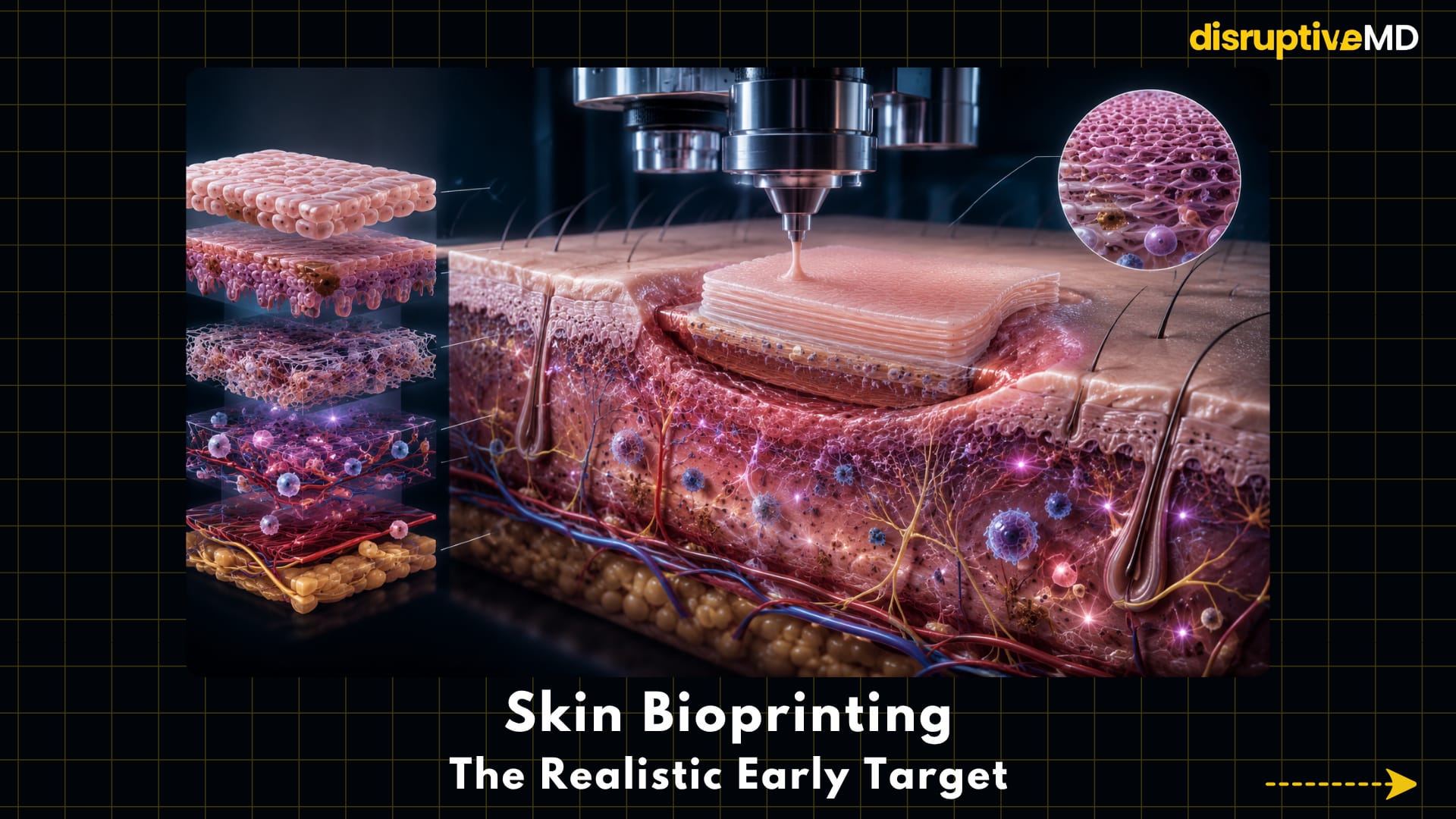
Skin Bioprinting: The Realistic Early Target
Skin is one of the most realistic early targets for bioprinting because it is relatively flat compared with complex internal organs.
That does not make it simple.
Skin is not just a sheet. It contains layers, blood vessels, immune cells, nerves, pigmentation, glands, hair follicles, extracellular matrix, and barrier function.
Still, compared with a kidney or lung, skin is more accessible. It can be monitored visually. It can be applied to wounds. It does not need to perform hundreds of internal metabolic functions.
Bioprinted skin could support future treatment of burns, chronic wounds, diabetic ulcers, trauma wounds, surgical wounds, skin disease models, cosmetic and toxicity testing
In the near term, bioprinted skin may be especially powerful as a research model and wound-healing platform.
The future version may go much further.
It may include multiple skin layers, vascular support, pigmentation, immune cells, nerves, sweat glands, and hair follicles. That would move bioprinted skin from a simple covering toward a more functional living tissue.
The challenge is not only closing a wound. The challenge is restoring living skin biology.
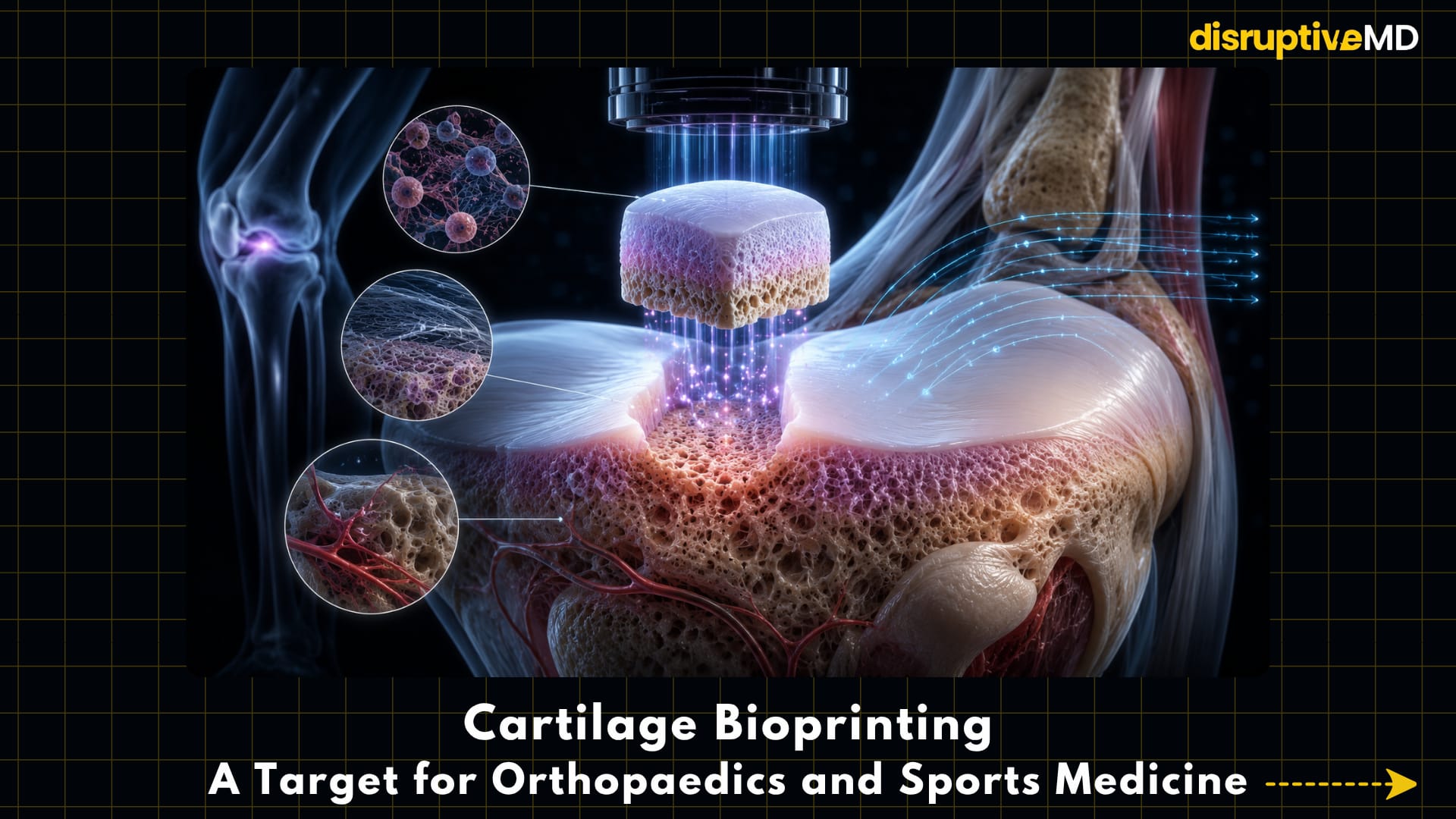
Cartilage Bioprinting: A Target for Orthopaedics and Sports Medicine
Cartilage is one of the most attractive targets for bioprinting because it has limited natural healing capacity.
Articular cartilage, the smooth tissue that covers joint surfaces, has no strong blood supply. Once damaged, it does not regenerate easily. That is why cartilage injuries can become chronic problems, especially in the knee, ankle, hip, and shoulder.
Bioprinting may help create cartilage-like structures for:
- Knee cartilage defects
- Injuries
- Ear cartilage
- Nasal cartilage
- Tracheal cartilage
- Joint repair research
For sports medicine and orthopaedics, the idea is powerful.
A patient with a cartilage defect may one day receive a custom-shaped living cartilage construct designed to match the defect and support joint mechanics.
But cartilage is harder than it looks.
Printed cartilage must be smooth, strong, durable, and able to survive repeated loading. It must integrate with the surrounding cartilage and underlying bone. It must maintain the right cell behaviour over time. It must not become weak, fibrotic, inflamed, or mechanically mismatched.
The future of cartilage bioprinting may not be a single printed plug. It may be multi-layered osteochondral repair: cartilage on top, bone-like support underneath, and a transition zone between them.
Bone Bioprinting: Building Strength and Biology Together
Bone is often described as hard tissue, but bone is alive.
It contains cells, blood vessels, marrow, minerals, collagen, signalling molecules, and a complex mechanical architecture. It remodels in response to stress. It heals after fractures. It communicates with the immune system and the metabolic system.
Bioprinting may support future repair of:
- Large bone defects
- Trauma injuries
- Tumor-related bone loss
- Spinal fusion research
- Jaw reconstruction
- Dental and craniofacial defects
- Orthopaedic scaffolds
The key challenge is the combination of biology and strength.
A soft cell-friendly material may support living cells but fail mechanically. A strong material may support load but fail biologically.
The ideal printed bone scaffold must do both. It must provide mechanical stability while also encouraging vascular ingrowth, bone-forming cell activity, and integration with the host skeleton. This is especially important in large defects, where the body may not be able to bridge the gap on its own.
The future may involve printed bone scaffolds that are patient-specific, porous, bioactive, and designed to guide the body’s own repair process.
Tendon and Ligament Bioprinting
Tendons and ligaments are difficult tissues to recreate because their structure is highly organised.
These tissues are not random ropes of collagen. They contain aligned fibres that transmit force in specific directions. They connect muscle to bone or bone to bone. They must tolerate tension, repetitive loading, and complex movement.
Bioprinting could help create tendon-like or ligament-like scaffolds that guide repair by controlling cell alignment, fibre direction, and mechanical architecture.
This is especially relevant for sports injuries, orthopaedic reconstruction, rotator cuff repair, ligament reconstruction, and tendon-bone interface repair
The tendon-bone interface is one of the most difficult regions to engineer because it is not one tissue. It transitions from tendon to fibrocartilage to mineralised tissue to bone.
A future bioprinted graft may need to reproduce that gradient. The real goal is not simply replacing a torn structure. It is restoring organised force transmission.
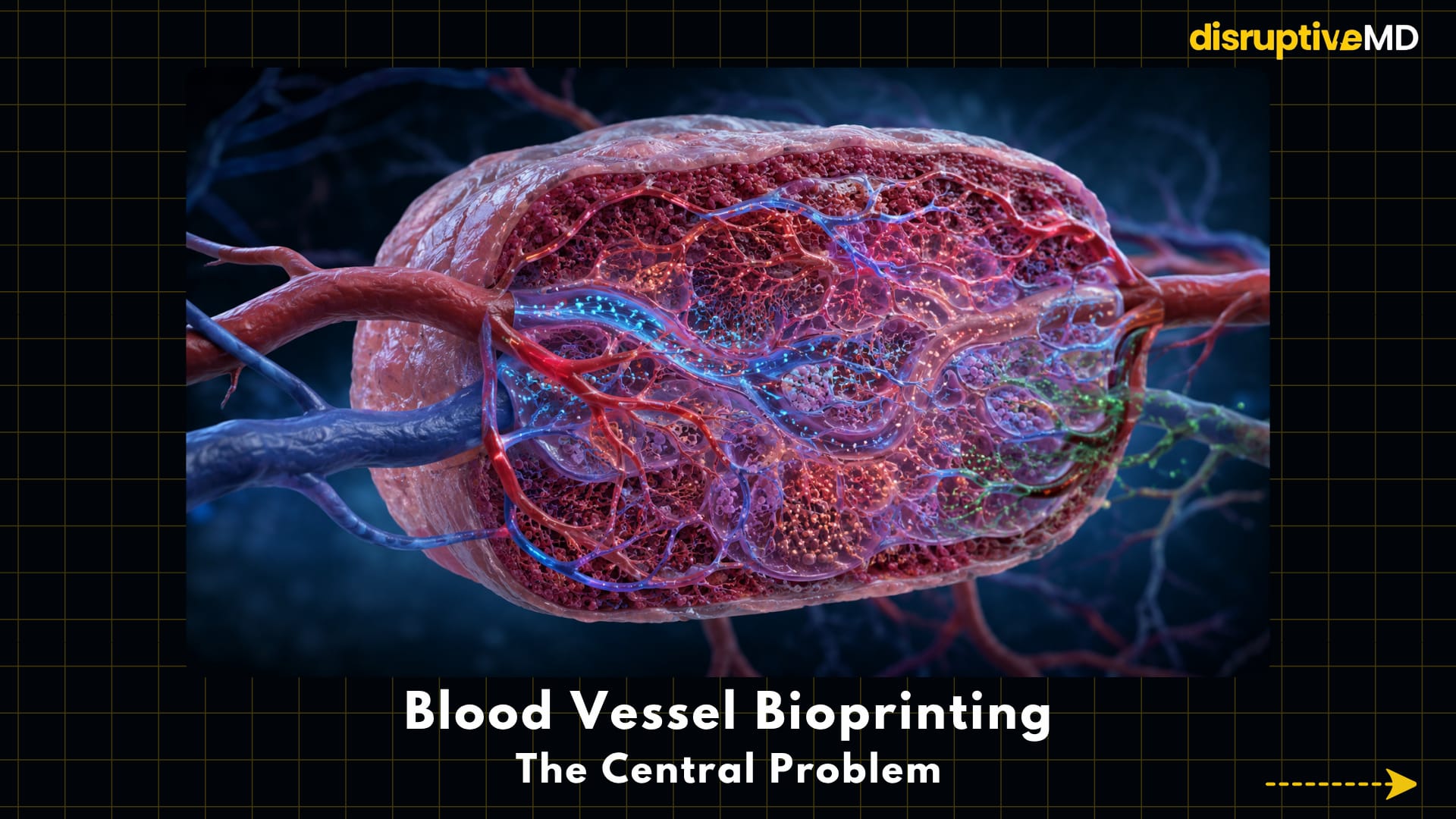
Blood Vessel Bioprinting: The Central Problem
Blood vessels are one of the most important challenges in bioprinting.
A tissue cannot survive if oxygen and nutrients cannot reach its cells. This is why vascularisation is the central problem in printing large tissues and organs.
Small tissue models can survive by diffusion for a limited distance. But thick tissues need a blood supply. Cells in the centre of a large printed structure can die if they do not receive oxygen, nutrients, and waste removal.
Bioprinting research is exploring:
- Printed vascular channels
- Microvascular networks
- Endothelial cells
- Perfusable tissue models
- Vascular graft research
- Sacrificial printing
- Microfluidics
- Organ-on-chip systems
Sacrificial printing is one clever strategy. A temporary material is printed inside a tissue construct and later removed, leaving behind channels that can carry fluid.
Microfluidics is another important direction. It allows tiny fluid channels to mimic aspects of blood flow, oxygen gradients, nutrient delivery, and drug exposure.
But true vascularisation is more than making tubes. A living organ needs large vessels, branching vessels, capillaries, oxygen exchange, nutrient delivery, waste removal, and connection to the patient’s own circulation.
This is why printing a full organ is much harder than printing an organ-shaped object.
The Vascularisation Problem
The vascularisation problem is the reason many people misunderstand bioprinting.
It is possible to print a shape that looks like an organ. It is much harder to print a living organ that behaves like one.
A full organ needs blood vessels at many scales: large vessels, branching vessels, small vessels, capillaries, oxygen exchange surfaces, nutrient delivery networks, and waste removal pathways.
The tissue must also survive the transition from printer to patient.
- It must tolerate handling.
- It must tolerate surgery.
- It must connect to blood flow.
- It must avoid clotting or leakage.
- It must maintain function under real biological pressure.
This is why a printed heart-shaped structure is not the same as a transplantable heart. The organ must live, integrate, and function. That is the true challenge.
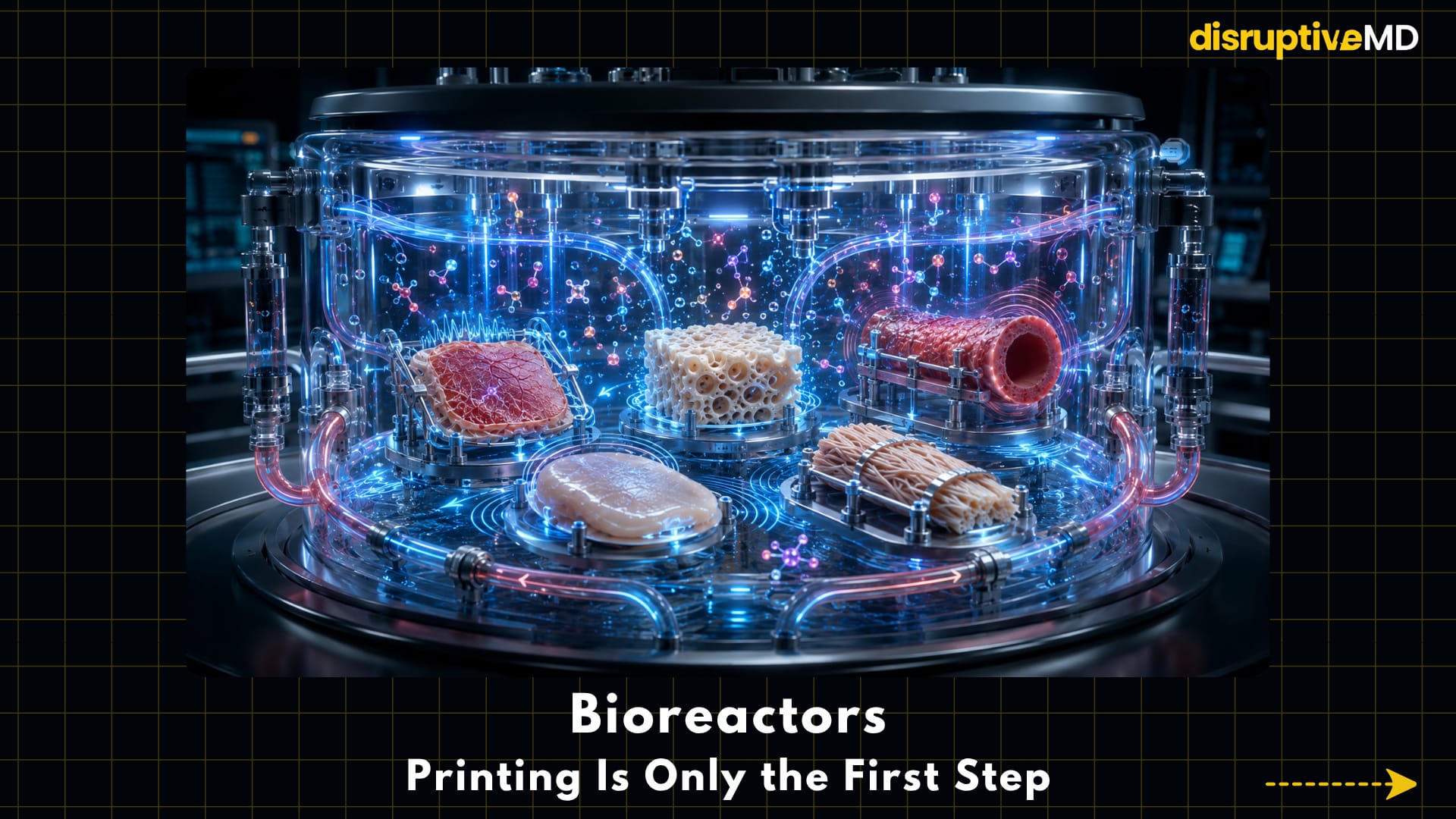
Bioreactors: Printing Is Only the First Step
One of the most important ideas in bioprinting is that printing may only be the beginning.
After printing, tissues may need to mature in a bioreactor.
A bioreactor is a controlled system that helps grow, train, and condition tissue after fabrication. It can provide nutrients, oxygen, mechanical stimulation, electrical stimulation, fluid flow, pressure, or biochemical signals.
Different tissues need different training.
- A printed heart patch may need rhythmic electrical stimulation.
- A printed bone scaffold may need mechanical loading.
- A printed vessel may need fluid flow.
- A printed cartilage structure may need compressive forces.
- A printed tendon scaffold may need tension and alignment cues.
This matters because cells do not become mature tissue simply because they are placed in the right shape. They need signals. They need time. They need mechanical and biochemical environments that teach them how to behave.
The future organ factory will not just print tissues. It will grow and train them.
Organoids and Mini-Organs
Organoids are small, simplified versions of organ-like tissue grown from cells.
They are not full organs. They do not fully reproduce the structure, scale, blood supply, or complete function of real organs. But they are extremely useful biological models.
Bioprinting can help arrange organoids or organoid-like structures in more controlled ways.
This can support disease modelling, drug testing, cancer research, toxicity testing, personalized medicine, developmental biology, and rare disease research.
Organoids are especially exciting because they can capture aspects of human biology that flat cell cultures may miss. A flat layer of cells in a dish is useful, but it does not fully mimic the 3D environment of the body. A bioprinted organoid model may allow cells to interact in more realistic spatial patterns. That could make research more human-relevant and more personalised.
The future may not be one organoid replacing one organ. It may be thousands of mini-tissues helping doctors and scientists understand disease before treating it.
Printed Liver Tissue Models
A fully transplantable printed liver is still far away.
But printed liver tissue models are already one of the most practical near-term uses of bioprinting.
The liver is central to drug metabolism, detoxification, protein synthesis, immune activity, and many other functions. This is why liver models are important for drug testing and toxicity research.
Traditional flat liver cell cultures often fail to fully capture real liver behaviour. Animal models can help, but they do not always predict human biology accurately.
Bioprinted liver tissue models may offer a more realistic platform.
They may help researchers study drug metabolism, toxicity, fatty liver disease fibrosis, inflammation, drug interactions, and personalized treatment response.
The key point is this: The first major impact of liver bioprinting may not be liver transplantation. It may be better drug testing.
Printed Tumour Models
Cancer is not just cancer cells.
A tumour includes extracellular matrix, blood vessels, immune cells, oxygen gradients, mechanical stiffness, signalling molecules, and complex interactions between different cell types.
That is why cancer can behave very differently in a flat dish compared with the human body.
3D bioprinting can create more realistic tumour models by arranging cancer cells, stromal cells, immune-related components, and matrix-like materials in controlled 3D environments.
This may help scientists study:
- How cancers grow
- How tumors invade
- How oxygen levels affect behavior
- How drugs penetrate tumor tissue
- How cancer cells interact with immune cells
- Why some tumours resist treatment
In the future, printed tumour models may support personalised oncology.
A patient’s tumour cells could potentially be used to create a model that tests how that tumour responds to different therapies. This does not mean every cancer patient will soon receive a printed tumour avatar. But it shows the field is heading from generic models toward patient-specific biology.
Organ-on-Chip Plus Bioprinting
Organ-on-chip systems use microfluidic devices to mimic aspects of organ function.
They do not recreate a whole organ. Instead, they use tiny channels, living cells, fluid flow, and controlled environments to model specific biological processes.
When organ-on-chip systems are combined with bioprinting, the result can be more powerful. Bioprinting can control tissue architecture. Microfluidics can control fluid flow. Cells can experience oxygen gradients, nutrients, drugs, and mechanical forces.
This combination may support drug testing, toxicity testing, disease modelling, immune interaction studies, personalised medicine, and reduced dependence on animal models.
*The goal is not to replace the entire human body on a chip. The goal is to build better human-relevant test systems. This is one of the most realistic near-term futures of bioprinting. *
Stem Cells and Induced Pluripotent Stem Cells
Stem cells are central to the future of bioprinting because printed tissue needs the right cell types.
Induced pluripotent stem cells are adult cells that have been reprogrammed into a more flexible state. In theory, they can be guided to become many different cell types. This could support patient-specific bioprinting.
A patient’s own cells could potentially be reprogrammed, expanded, differentiated, and used to create tissue models or repair constructs. This may reduce immune mismatch and allow more personalised disease modelling.
But the challenges are serious.
- Cells must differentiate correctly.
- They must mature properly.
- They must behave safely.
- They must not become abnormal.
- They must remain stable over time.
- They must perform the function required by the tissue.
A cell that looks correct in the lab may still behave differently inside the body. This is why stem-cell-based bioprinting is exciting but must be handled with scientific caution.
Decellularised Extracellular Matrix
One exciting bioink strategy uses decellularised extracellular matrix. This means taking tissue, removing the cells, and using the remaining structural and biochemical matrix as a tissue-specific material.
The idea is simple but powerful.
Cells do not live in empty space. They live inside an extracellular matrix - a complex environment that provides structure, signals, stiffness, and biochemical cues.
A decellularised matrix may help give printed cells a more natural environment.
Examples include heart-derived matrix for heart tissue, cartilage-derived matrix for cartilage, liver-derived matrix for liver models, and skin-derived matrix for skin repair.
This approach may help printed cells behave more like they would in the original tissue.
But it also raises challenges.
The material must be processed safely. It must be consistent. It must be printable. It must not carry unwanted biological material. It must support the right mechanical properties.
The promise is tissue-specific biology. The challenge is controlled manufacturing.
Smart Bioinks
Future bioinks may not be passive gels.
They may be smart materials that respond to their environment.
Smart bioinks could respond to temperature, pH, enzymes, mechanical stress, electrical signals, light, inflammation, and healing signals.
This could allow printed tissues to change over time.
- A smart bioink might release growth factors when needed.
- It might stiffen or soften during healing.
- It might guide cell migration.
- It might degrade as new tissue forms.
- It might help cells mature in response to mechanical loading.
This is where bioprinting becomes more than construction. It becomes biological programming. The printed tissue is not only placed into the body. It is designed to interact with the body.
Multi-Material Bioprinting
Real tissues are not made from one material.
Bone, cartilage, blood vessels, nerves, fat, muscle, and skin all have different stiffness, cell types, and architecture.
A single-material print cannot easily recreate this complexity.
Multi-material bioprinting aims to print different materials and cell types within the same construct.
This is essential for complex tissues.
- A joint surface may need cartilage, calcified cartilage, bone, and vascular support.
- A skin construct may need epidermal and dermal layers.
- A heart patch may need muscle cells, vascular cells, matrix support, and electrical coordination.
- A tendon-bone repair may need a gradient from soft tendon to hard bone.
The future of bioprinting is not one bioink making one tissue. It is multiple bioinks, multiple cell types, and multiple structural zones working together.
Bioprinting and AI
Artificial intelligence could become a major accelerator for bioprinting.
Bioprinting involves too many variables for simple trial and error.
- Bioink composition matters.
- Cell density matters.
- Printing pressure matters.
- Nozzle size matters.
- Temperature matters.
- Crosslinking matters.
- Tissue geometry matters.
- Vascular channel placement matters.
- Mechanical stiffness matters.
- Bioreactor conditions matter.
AI could help optimise these variables.
It may help answer:
- Which bioink composition is best?
- Which cell density is ideal?
- Which structure will survive after printing?
- Where should vascular channels go?
- How will the tissue mature?
- Will the construct deform after implantation?
- Which design is most likely to integrate?
AI may also support defect detection during printing. A bioprinter could use imaging and sensors to detect structural errors, cell distribution problems, or print instability.
This creates a powerful link between regenerative medicine, digital twins, robotics, and biofabrication. The future organ factory may be partly biological and partly computational.
Digital Twins of Tissues
Before printing a tissue, scientists may one day simulate it digitally.
A digital twin could model:
- Tissue geometry
- Mechanical stress
- Nutrient diffusion
- Oxygen delivery
- Vascular flow
- Cell growth
- Tissue maturation
- Implant integration
This could help improve the design before the tissue is printed.
For example, a digital model could predict whether the centre of a printed tissue will receive enough oxygen. It could test where vascular channels should be placed. It could estimate how a cartilage scaffold will respond to loading. It could predict whether a tissue patch will deform after implantation.
This is the future link between digital medicine and regenerative medicine. A tissue may be designed virtually, tested computationally, printed biologically, matured physically, implanted surgically, and monitored clinically.
In-Situ Bioprinting
In-situ bioprinting means printing directly onto or into the patient’s body.
Instead of printing a tissue outside the body and implanting it later, a printer could deposit cells and biomaterials directly at the injury site.
This is especially interesting for:
- Wounds
- Burns
- Cartilage defects
- Bone defects
- Surgical repair
- Soft-tissue reconstruction
For example, a skin printer could theoretically deposit layers of bioink directly over a burn wound. A surgical bioprinter could deposit biomaterial into a cartilage defect. A robotic system could help guide printing during an operation.
This idea is futuristic and exciting.
But it also raises major questions.
- How do we maintain sterility?
- How do we print accurately on living tissue that moves and bleeds?
- How do we control cell survival?
- How do we avoid infection?
- How do we ensure the bioink stays where it is placed?
- How do we regulate a procedure where manufacturing happens inside the body?
In-situ bioprinting may become one of the most dramatic forms of regenerative surgery. But it will require extreme precision and safety.
Bioprinted Patches Before Full Organs
The first clinically useful bioprinted therapies may not be full organs.
They may be patches.
This is a more realistic near-term pathway.
Examples include:
- Heart repair patches
- Cartilage repair patches
- Skin wound patches
- Liver tissue patches
- Vascularised tissue patches
- Bone defect scaffolds
- Nerve repair guides
A patch does not need to replace the entire organ. It only needs to support repair, restore a local function, or improve healing.
That makes it more achievable.
- A heart patch may support damaged muscle.
- A cartilage patch may fill a defect.
- A skin patch may support wound closure.
- A bone scaffold may guide regeneration.
- A liver tissue patch may support research before replacement.
- A vascularised patch may help reconstruct complex tissue loss.
This is where the organ factory may begin. Not with a printed heart. But with a printed piece of living repair.
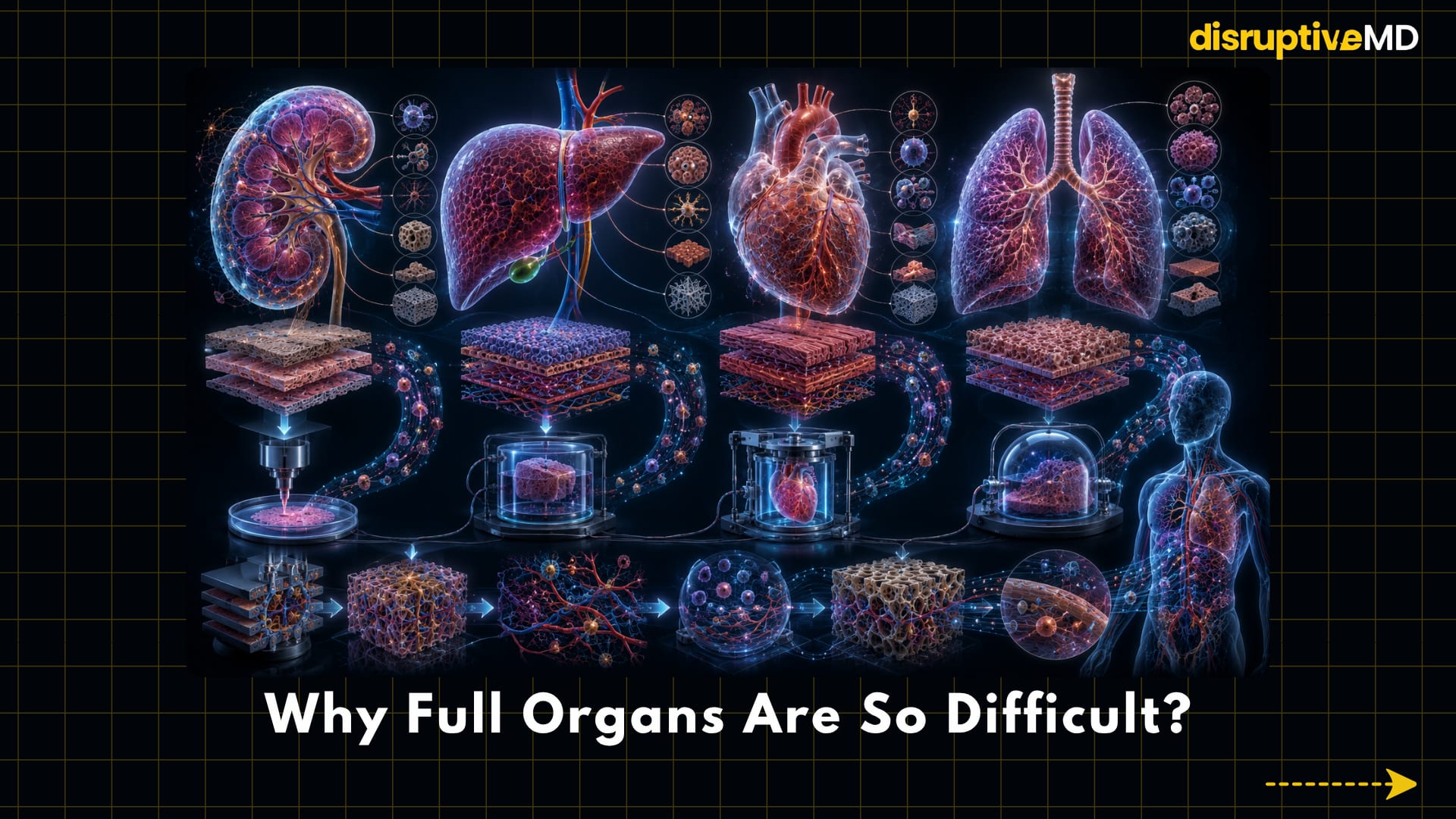
Why Full Organs Are So Difficult
A full organ is not just a 3D structure.
It needs:
- multiple cell types
- blood vessels
- nerves
- immune compatibility
- mechanical strength
- correct shape
- correct function
- oxygen delivery
- waste removal
- tissue maturation
- integration with the body
- long-term safety
- surgical implantability
That is why printing a kidney, liver, heart, or lung is one of the hardest goals in regenerative medicine.
Each organ has its own unique biology.
- A kidney filters blood and manages fluid, electrolytes, waste, hormones, and urine drainage.
- A liver performs metabolic, detoxification, immune, synthetic, and regenerative functions.
- A heart is an electrically coordinated pump that must contract rhythmically under pressure.
- A lung exchanges gases across a massive delicate surface while maintaining airways, vessels, elasticity, and immune defence.
Printing these organs requires more than anatomy. It requires function at scale. That is why full organ bioprinting remains a long-term goal, not a routine clinical reality.
Immune Compatibility
Even if a tissue is printed perfectly, the body may reject it or react against it.
Using a patient’s own cells may reduce immune mismatch, but it does not solve every problem.
- Biomaterials can trigger inflammation.
- Scaffold residues may affect safety.
- Cells may be immature.
- Cells may behave unpredictably.
- Contamination is a risk.
- Abnormal tissue growth is a concern.
- The immune system may react to the construct after implantation.
This is why immune compatibility is not just about the cell source. It is about the entire biological product. A printed tissue must be safe, stable, clean, functional, and accepted by the body.
Manufacturing and Quality Control
Bioprinted tissues are living products.
That makes quality control much harder than ordinary implant manufacturing.
- A metal implant can be tested for shape, strength, surface finish, and material properties.
- A living tissue must be tested for far more.
Every product may need evaluation for sterility, cell viability, cell identity, genetic stability, mechanical strength, biological activity, vascular function, reproducibility, batch consistency, and long-term behaviour.
This is especially challenging for patient-specific tissues. If every tissue is custom-made, then every tissue may be slightly different. That creates a major manufacturing problem.
How do you prove that a living product is consistent when the product is personalized? This question will define the future of clinical bioprinting.
Regulation and Safety
Bioprinted tissues may fall between categories.
- Are they medical devices?
- Are they biologics?
- Are they tissue products?
- Are they combination products?
- Are they surgical materials?
- Are they personalised living medicines?
The answer may depend on the cells, biomaterials, manufacturing process, intended use, and level of manipulation.
Before clinical use, regulators must understand:
- What exactly is the product?
- What cells are used?
- What biomaterials are used?
- How is it manufactured?
- How is quality tested?
- How long does it survive?
- What are the risks?
- Can it form abnormal tissue?
- Can it fail mechanically?
- Can it trigger immune reactions?
This is why regulation is not a barrier to innovation.
It is part of making the innovation safe enough to use in real patients.
Ethical Questions
The organ factory idea also raises important ethical questions.
- Who owns a bioprinted tissue made from a patient’s cells?
- Could it be used for research?
- Could it be commercialised?
- Who gets access first?
- Will it be affordable?
- How do we prevent unproven clinics from selling fake “printed organ” therapies?
- Should complex living tissues be treated like products, organs, or something new?
These questions matter because the future of bioprinting will not only be technical. It will be social, economic, legal, and ethical.
Fact Base
3D bioprinting can create tissue-like structures by combining cells, biomaterials, and printing technologies.
Bioinks are central to the field because they determine printability, cell survival, mechanical behaviour, and biological function.
Skin, cartilage, bone, blood vessels, tendon-like tissues, tumour models, liver models, organoids, and tissue patches are active areas of research.
Bioprinted tissue models are especially useful for drug testing, toxicity testing, disease modelling, and personalised research.
Vascularisation remains one of the biggest unsolved problems because large tissues need blood vessels for oxygen delivery, nutrient supply, and waste removal.
Bioreactors may be necessary after printing because tissues often need time, flow, oxygen, mechanical stimulation, electrical stimulation, or biochemical cues to mature.
Patient-specific bioprinting could use imaging data to design personalised tissue constructs.
In-situ bioprinting could one day allow cells and biomaterials to be deposited directly at injury sites, but safety and precision challenges remain significant.
Printed patches and scaffolds are more realistic near-term applications than full transplantable organs.
Full organs remain extremely difficult because they require multiple cell types, vascular networks, nerves, immune compatibility, mechanical strength, maturation, integration, and long-term function.
Bioprinted tissues will require strict quality control because they are living products, not ordinary manufactured devices.
The future of bioprinting will require collaboration between tissue engineers, surgeons, biologists, materials scientists, AI researchers, regulators, ethicists, and clinicians.
What Is Possible Today
3D bioprinting can create tissue-like structures.
Skin, cartilage, bone, vascular models, tumour models, liver models, and organoids are active research areas.
Bioprinted tissues are useful for drug testing and disease modelling.
Patient-specific tissue repair is a realistic long-term direction.
Bioprinted patches and scaffolds are more realistic than full organs in the near term.
What is not fully real yet:
- Routine printing of transplantable hearts
- Routine printing of transplantable kidneys
- Routine printing of transplantable livers
- Fully functional printed lungs
- Hospital-based organ factories for everyday clinical care
- Guaranteed immune-safe printed organs
- Large-scale affordable manufacturing of living replacement organs
This difference is important. The hype says: “We will print organs soon.” The science says: “We are learning how to print living tissues, and that may slowly build toward organ-level repair.”
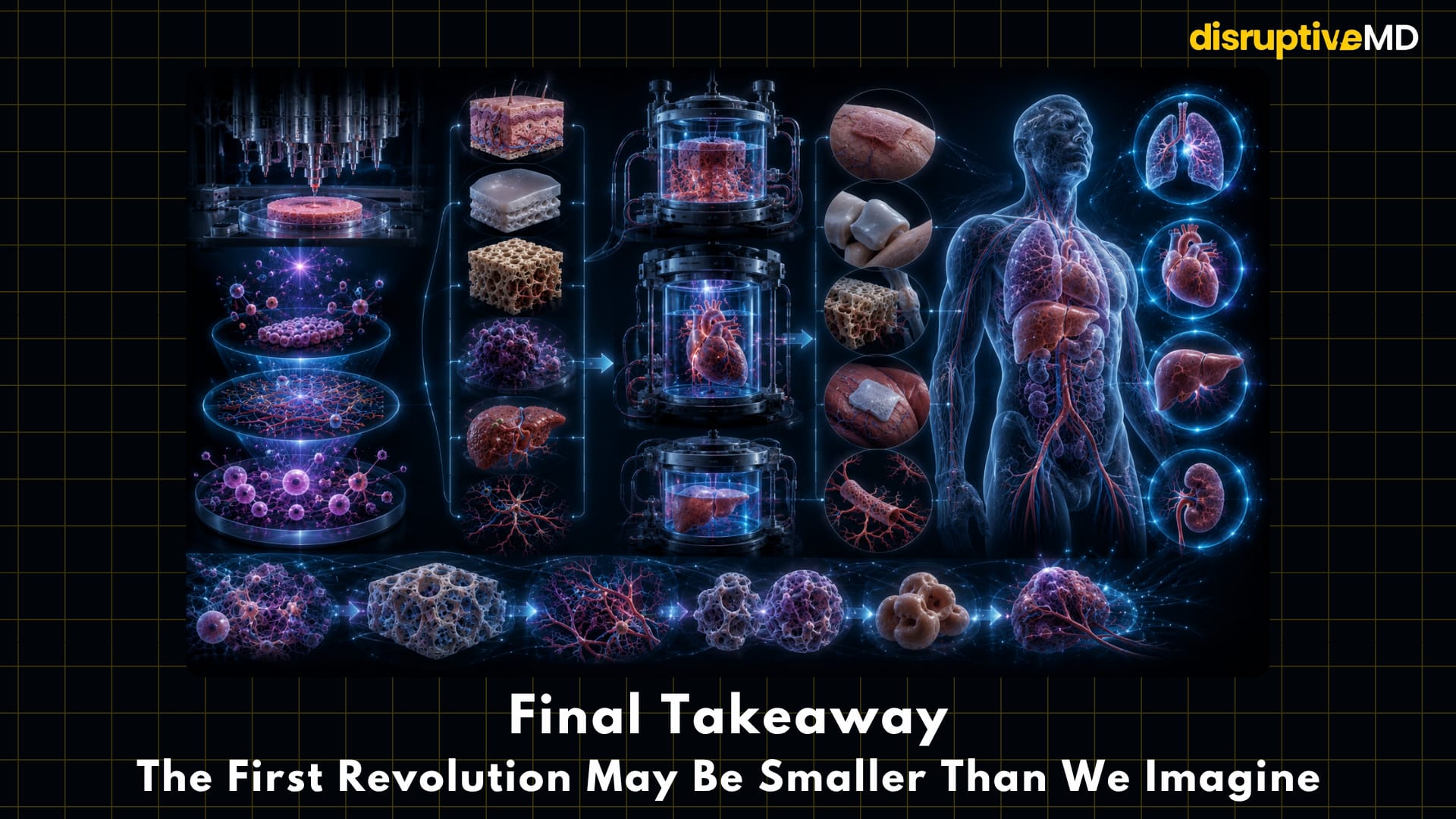
Conclusion: The First Revolution May Be Smaller Than We Imagine
The future organ factory is one of the most exciting ideas in medicine.
It imagines a world where damaged tissues are not only repaired, replaced, or supported, but are manufactured biologically.
A burn wound could receive printed skin.
A cartilage defect could receive a patient-shaped living patch.
A bone defect could receive a bioactive scaffold.
A tumour could be modelled outside the body before treatment.
A liver-like tissue could help test drug toxicity.
A heart patch could support damaged muscle.
The journey from printed tissue models to transplantable organs will require breakthroughs in vascularisation, cell maturation, immune safety, mechanical strength, quality control, regulation, and long-term function.
3D bioprinting is the slow engineering of living biology. And if it succeeds, the future hospital may not only treat tissue failure - It may manufacture repair.
References
- Kazemi M, Maralbashi S. Advances in 3D bioprinting for medical application: opportunities and challenges.BioMedical Engineering OnLine. 2025/2026;25:11. DOI: https://doi.org/10.1186/s12938-025-01498-y
- Gungor-Ozkerim PS, Inci I, Zhang YS, Khademhosseini A, Dokmeci MR. Bioinks for 3D bioprinting: an overview. Biomaterials Science. 2018;6:915–946. DOI: https://doi.org/10.1039/C7BM00765E
- Chen EP, Toksoy Z, Davis BA, Geibel JP. 3D Bioprinting of Vascularized Tissues for in vitro and in vivo Applications. Frontiers in Bioengineering and Biotechnology. 2021;9:664188. DOI: https://doi.org/10.3389/fbioe.2021.664188
- Douglas A, Chen Y, Elloso M, Levschuk A, Jeschke MG. Bioprinting-By-Design of Hydrogel-Based Biomaterials for In Situ Skin Tissue Engineering. Gels. 2025;11(2):110. DOI: https://doi.org/10.3390/gels11020110
- Bai X, Yang Y, Chu J, Deng Y, Li M, Yang H. 3D bioprinting patient-specific grafts for tendon/ligament repair in motion: emerging trends and challenges. Frontiers in Bioengineering and Biotechnology. 2025;13:1643430. DOI: https://doi.org/10.3389/fbioe.2025.1643430
- Mallya D, Gadre MA, Varadharajan S, Vasanthan KS. 3D bioprinting for the construction of drug testing models-development strategies and regulatory concerns. Frontiers in Bioengineering and Biotechnology.2025;13:1457872. DOI: https://doi.org/10.3389/fbioe.2025.1457872
- Huang J, Xiong J, Wang D, Zhang J, Yang L, Sun S, Liang Y. 3D Bioprinting of Hydrogels for Cartilage Tissue Engineering. Gels. 2021;7(3):144. DOI: https://doi.org/10.3390/gels7030144
- Potyondy T, Uquillas JA, Tebon P, Byambaa B, Hasan A, Tavafoghi M, Marycz K, Aninwene GE, Khademhosseini A, Nasajpour A. Recent advances in 3D bioprinting of musculoskeletal tissues. Biofabrication.2021;13(2):022001. DOI: https://doi.org/10.1088/1758-5090/abc8de
- Xu J, Li W, Liu Y, Zhang X, Chen X, Deng C, Zhang J. 3D Printing for Bone-Cartilage Interface Regeneration.Frontiers in Bioengineering and Biotechnology. 2022;10:828921. DOI: https://doi.org/10.3389/fbioe.2022.828921
- Weng T, Zhang W, Xia Y, Wu P, Yang M, Jin R, Xia S, Wang J, You C, Han C, Wang X. 3D bioprinting for skin tissue engineering: Current status and perspectives. Journal of Tissue Engineering.2021;12:20417314211028574. DOI: https://doi.org/10.1177/20417314211028574 Regulatory / background sources used
- U.S. Food and Drug Administration. Technical Considerations for Additive Manufactured Medical Devices: Guidance for Industry and Food and Drug Administration Staff. No DOI. Official FDA guidance.
- U.S. Food and Drug Administration. Focus Area: Regenerative Medicine. No DOI. Official FDA regulatory science resource.
- U.S. Food and Drug Administration. Cellular & Gene Therapy Guidances. No DOI. Official FDA guidance index.
- U.S. Food and Drug Administration. 3D Printing of Medical Devices. No DOI. Official FDA medical device resource.