
What if a tumour could be destroyed with extreme cold while MRI watches the treatment in real time?
Cancer treatment has traditionally depended on three major approaches: removing a tumour surgically, destroying it with radiation, or attacking it with systemic drugs.
MRI-guided cryoablation introduces another possibility.
Instead of removing the tumour through a large incision, clinicians insert one or more thin cryoprobes directly into it. These probes generate extremely low temperatures, creating a controlled zone of frozen tissue around the tumour.
MRI is then used to guide probe placement, visualise the surrounding anatomy and monitor the expanding region of ice during treatment.
The goal is simple but powerful: Destroy the selected tumour while causing as little damage as possible to the rest of the body.
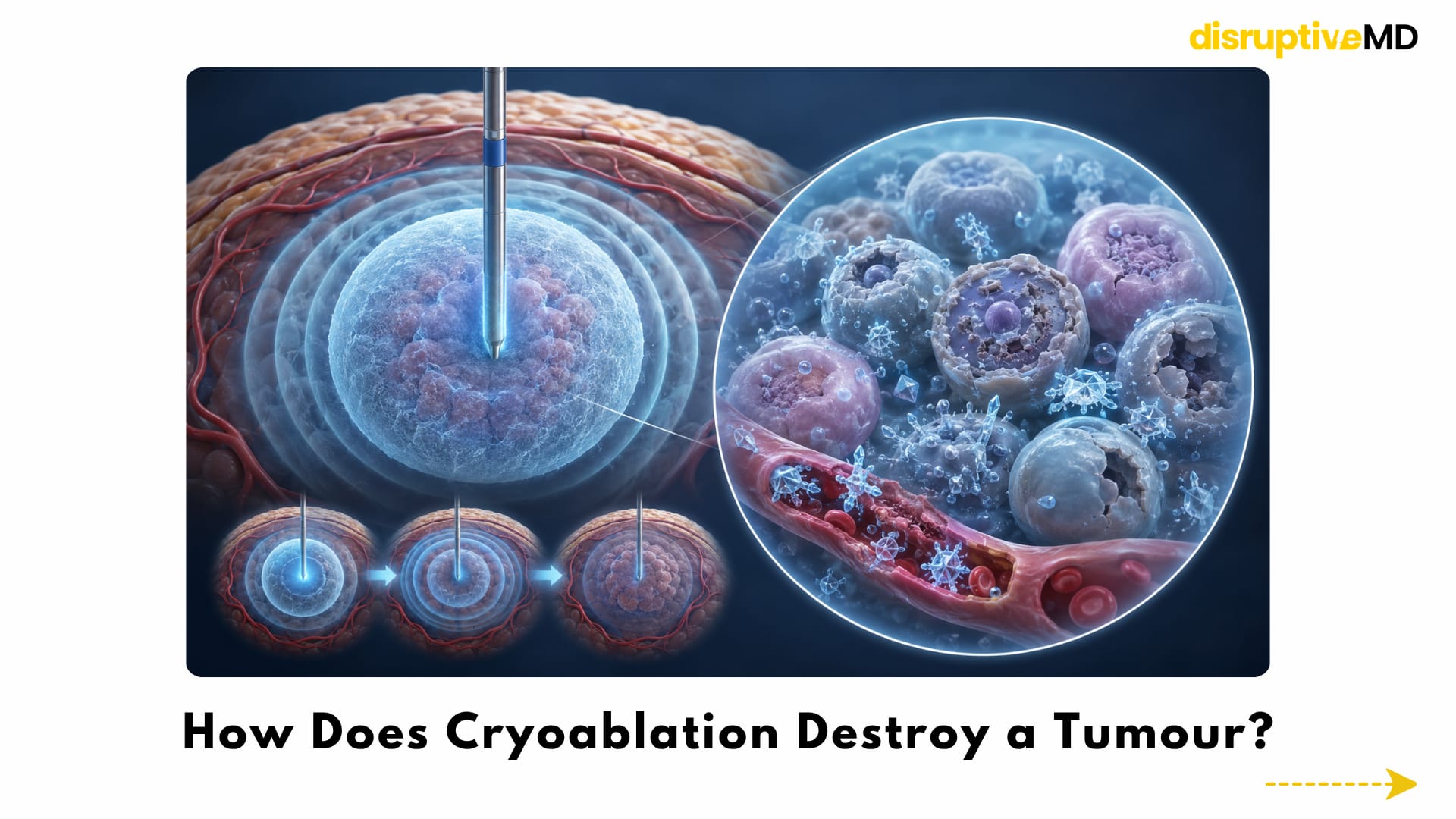


- Gas circulating through the cryoprobe rapidly removes heat from the surrounding tissue.
- As the temperature falls, ice crystals form inside and outside tumour cells. Cell membranes become damaged, proteins and cellular structures are disrupted, and small blood vessels supplying the treated tissue are injured.
- Repeated freezing and thawing strengthens the biological injury and helps create irreversible cell death within the target zone.
HOW DOES CRYOABLATION DESTROY A TUMOUR?
Cryoablation does more than simply make tissue cold.
Gas circulating through the cryoprobe rapidly removes heat from the surrounding tissue. As the temperature falls, ice crystals form inside and outside tumour cells. Cell membranes become damaged, proteins and cellular structures are disrupted, and small blood vessels supplying the treated tissue are injured.
The tumour is usually exposed to controlled freeze-and-thaw cycles. Repeated freezing and thawing strengthens the biological injury and helps create irreversible cell death within the target zone.
Because the probes are placed through small skin punctures, the treatment can avoid the tissue disruption associated with a major surgical incision.
However, cryoablation is still an invasive medical procedure. Bleeding, infection, injury to nearby nerves or organs, skin damage and incomplete tumour destruction remain possible risks.
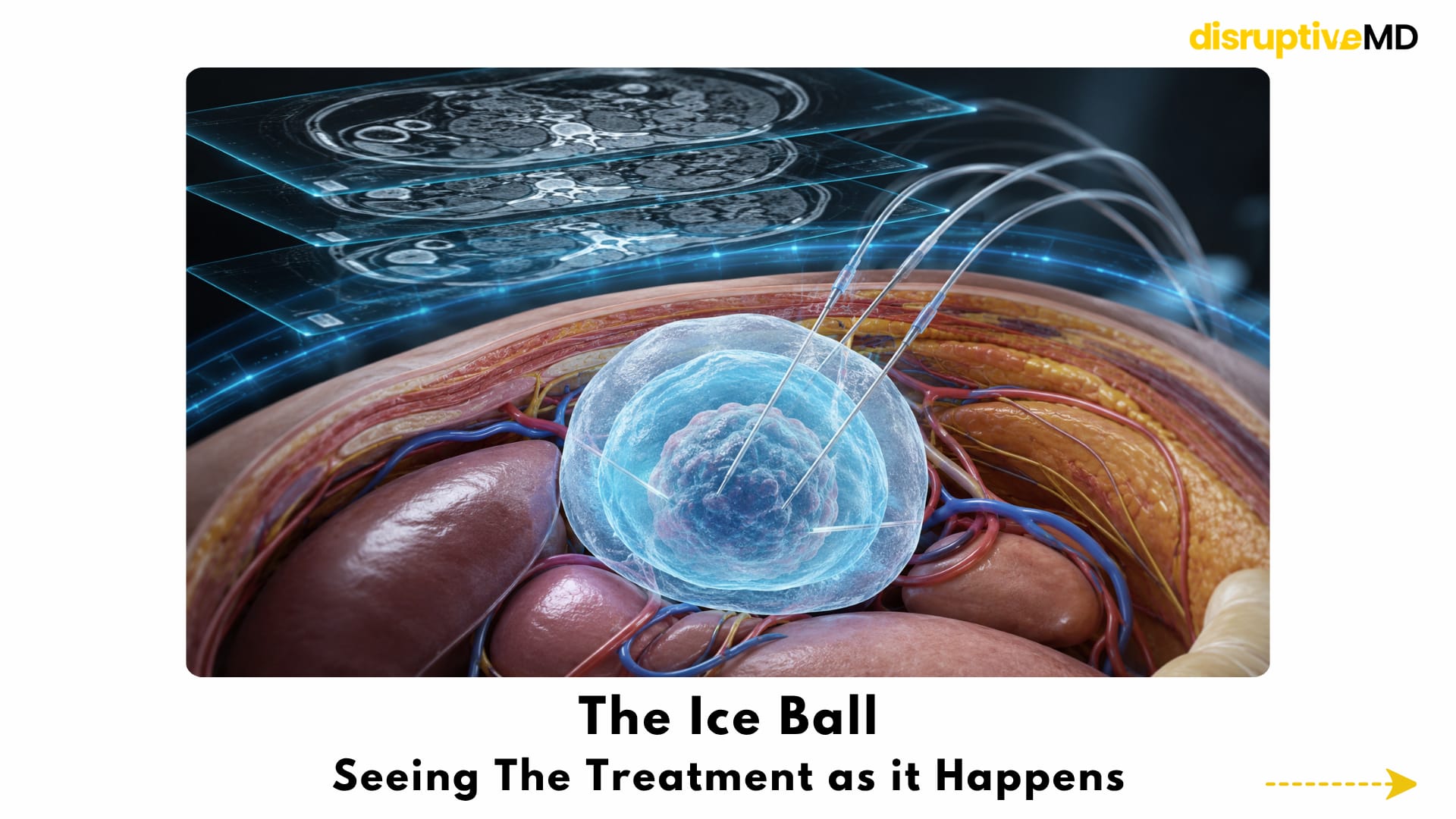
THE ICE BALL: SEEING THE TREATMENT AS IT HAPPENS
One of the most important features of cryoablation is the formation of an ice ball.
As freezing begins, a visible zone of frozen tissue develops around each probe. Multiple probes can be positioned together to create an ice ball shaped around the tumour.
The aim is not merely to touch the tumour with ice. The ice ball must extend beyond the visible tumour boundary to create an appropriate treatment margin.
A critical detail is that the outer edge of the visible ice ball is not necessarily cold enough to kill every cell. Lethal temperatures occur deeper inside the frozen zone. The operator must therefore plan enough extension beyond the tumour while protecting nearby organs, nerves, blood vessels, skin and other vulnerable structures.
This balance between coverage and protection is where imaging becomes central to the procedure.
WHY MRI GUIDANCE MATTERS
Computed tomography and ultrasound are more widely used for many cryoablation procedures. MRI guidance is particularly valuable when superior soft-tissue visibility or multiplanar imaging is needed.
MRI can help clinicians:
- identify tumours that are difficult to distinguish on non-contrast CT
- visualise the tumour in several imaging planes
- examine its relationship with vessels, nerves and surrounding organs
- guide cryoprobes toward deep or difficult targets
- monitor the developing ice ball during freezing
- avoid ionising radiation during the procedure
The ice ball usually appears as a clearly defined low-signal region on MRI, allowing the treatment team to repeatedly assess its size and position. Real-time and near-real-time MRI techniques have demonstrated that probe placement and ice-ball growth can be monitored inside clinical MRI systems.
MRI guidance also has limitations. MRI-compatible equipment is required, access inside the scanner can be restricted, metal probe artefacts may interfere with visibility, and the procedures can take longer than CT-guided cryoablation. Interventional MRI facilities are also available in relatively few centres.
KIDNEY TUMOURS: AN IMPORTANT CLINICAL USE CASE
Small renal tumours are among the strongest clinical examples of MRI-guided cryoablation.
Preserving functioning kidney tissue can be particularly important in older patients, people with impaired kidney function, patients with multiple medical conditions or those considered high-risk candidates for surgery.
During renal cryoablation, probes are placed into the tumour while the remaining kidney is preserved as much as possible. MRI can be especially useful for endophytic or intraparenchymal tumours that are difficult to see clearly with CT or ultrasound.
Long-term observational studies have reported favourable local control in carefully selected patients with small renal cell carcinomas. A large study of CT- and MRI-guided cryoablation also reported strong intermediate- and long-term outcomes, although the results came from specialised centres and should not be interpreted as proof that ablation is appropriate for every renal tumour.
The decision between active surveillance, partial nephrectomy and ablation depends on tumour size, tumour position, kidney function, age, surgical risk, biopsy findings and the patient’s wider clinical situation.
BONE, SPINE AND SOFT-TISSUE TUMOURS Cryoablation is also being used for selected bone and soft-tissue tumours.
In patients with painful bone metastases, treatment may be performed to reduce pain and improve quality of life rather than to cure the underlying cancer. The multicentre MOTION study reported rapid and durable pain improvement following image-guided cryoablation in appropriately selected patients with painful bone metastases.
MRI guidance becomes particularly interesting when a tumour lies near the spinal canal, nerves or other delicate soft-tissue structures. Small clinical reports have demonstrated MRI monitoring of cryoablation in selected epidural and spinal malignancies, where visualising the boundary between the ice ball and neural structures is essential.
In soft-tissue tumours, cryoablation may be used for local tumour control, symptom relief or treatment of selected recurrent and difficult-to-operate lesions. These applications remain highly dependent on tumour biology, size, anatomical location and multidisciplinary assessment.
PROSTATE, BREAST AND OTHER TUMOURS
The broader field of image-guided cryoablation extends beyond kidney and musculoskeletal tumours, although MRI is not necessarily the main guidance method in every organ.
In prostate cancer, MRI information can be fused with real-time ultrasound to guide focal cryoablation toward the known tumour while attempting to preserve surrounding prostate tissue. Early and intermediate results are encouraging in selected patients, but long-term cancer control and reliable detection of residual disease remain important concerns.
Breast cryoablation is commonly performed with ultrasound rather than continuous MRI guidance. The five-year ICE3 study evaluated cryoablation without surgical excision in women aged 60 years or older with carefully selected, low-risk early breast cancers. The results support continued investigation, but they do not establish cryoablation as a universal replacement for breast-conserving surgery.
Cryoablation is also used or investigated in selected liver, lung and other solid tumours. In these organs, CT, ultrasound, fusion imaging or combinations of imaging techniques may be more practical than fully MRI-guided treatment.
The important distinction is that cryoablation is the treatment technology, while MRI is one possible guidance and monitoring platform.
THE IMMUNE SYSTEM ANGLE
Freezing may have effects beyond the tissue immediately surrounding the cryoprobe.
When tumour cells are destroyed, tumour-associated proteins and antigens can be released into the local environment. Researchers are investigating whether this material can help immune cells recognise the cancer more effectively.
This has created interest in combining cryoablation with immune-checkpoint inhibitors and other immunotherapies.
However, the immune response to freezing is complex. Cryoablation may produce both immune-stimulating and immune-suppressing signals. Most evidence supporting a powerful systemic or “abscopal” effect remains preclinical or based on small, early clinical studies.
Cryoablation should therefore not currently be described as a reliable cancer vaccine or a proven way of eliminating untreated tumours elsewhere in the body.
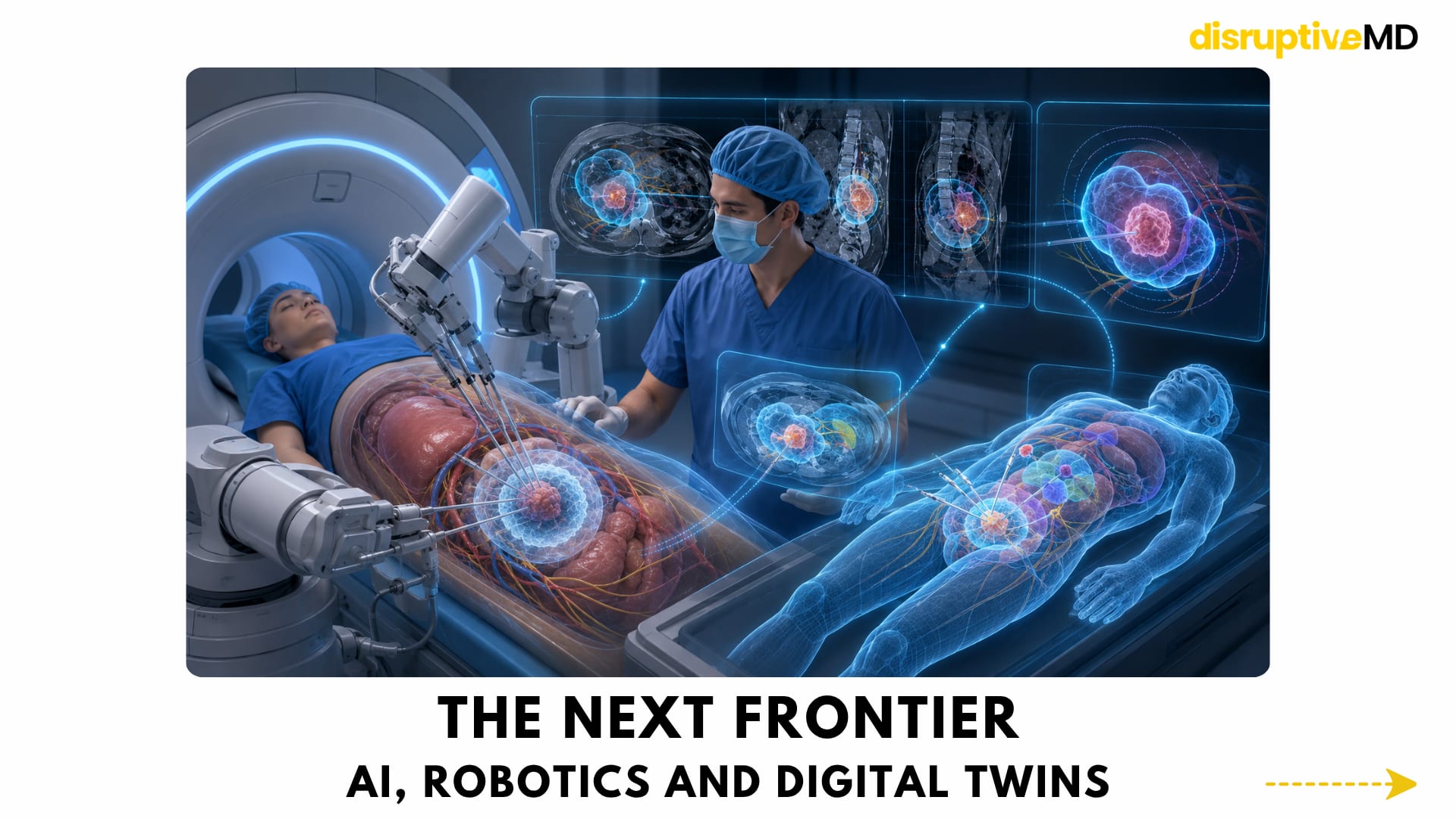
THE NEXT FRONTIER: AI, ROBOTICS AND DIGITAL TWINS
The future of cryoablation may involve a much more intelligent treatment environment.
AI systems could potentially segment the tumour automatically, map nearby structures and calculate whether the developing ice ball is likely to achieve an adequate margin.
Robotic systems could assist with stable, geometrically precise probe placement—particularly when several probes must be positioned around an irregular tumour.
A patient-specific digital model could simulate:
- the number and position of cryoprobes
- the expected shape of the ice ball
- freeze-and-thaw duration
- lethal temperature boundaries
- blood-vessel heat effects
- safety distances from nerves and organs
- the probability of incomplete tumour coverage
This would transform treatment planning from relying mainly on probe experience and standard manufacturer predictions to using a personalised simulation of how freezing may behave inside an individual patient.
These technologies are plausible research directions, but fully automated MRI-guided cryoablation and clinically validated cryoablation digital twins are not routine cancer treatments today. Read more about digital twins Read more about robotics
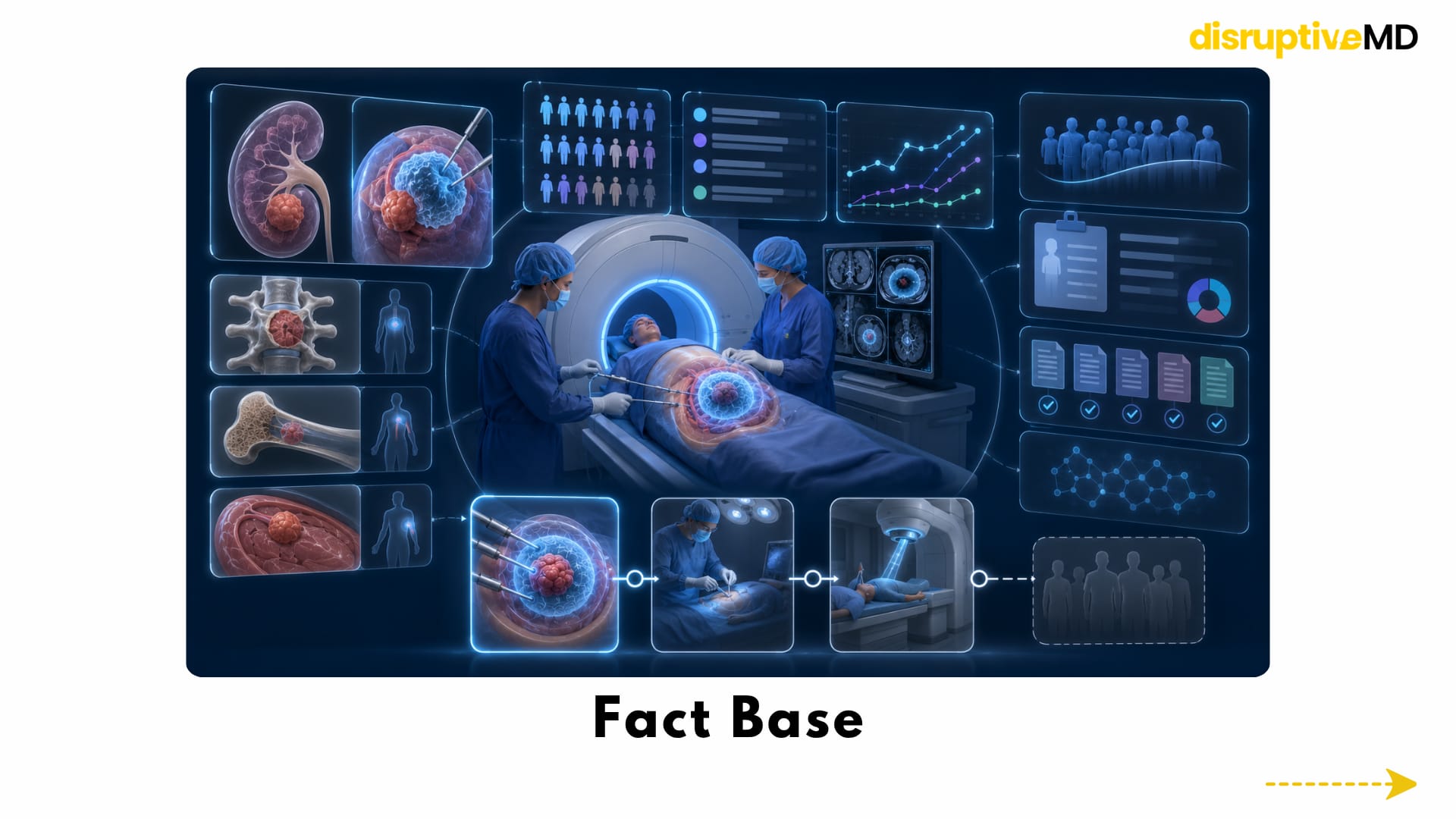
FACT BASE
MRI-guided cryoablation is a real minimally invasive treatment performed in specialist interventional oncology centres.
Its strongest clinical support is currently found in selected small renal tumours, with additional applications in carefully chosen bone, spine and soft-tissue lesions.
The technology offers several important advantages:
- small percutaneous access points
- detailed soft-tissue imaging
- multiplanar treatment planning
- direct visualisation of ice-ball growth
- preservation of surrounding tissue when technically possible
- the possibility of repeating treatment in selected cases
- no ionising radiation from MRI guidance
However, most published evidence consists of retrospective studies, specialist-centre series, single-arm trials and selected patient populations. Direct randomised comparisons with surgery or radiotherapy remain limited for many tumour types.
WHAT IS POSSIBLE TODAY?
MRI-guided cryoablation can provide meaningful local tumour control or symptom relief in carefully selected patients.
It is particularly relevant when:
- the tumour can be reached safely with a percutaneous probe
- preserving an organ is clinically important
- major surgery carries substantial risk
- the target is difficult to see clearly using CT or ultrasound
- detailed monitoring near critical soft-tissue structures is required
- local palliation is needed for painful metastatic disease
Patient selection, biopsy information, tumour biology, imaging visibility, adequate ablation margins and long-term follow-up remain essential.
WHAT IS NOT FULLY REAL YET?
MRI-guided cryoablation is not suitable for every tumour, patient or anatomical location.
It does not universally replace surgery, chemotherapy, radiotherapy, targeted therapy or immunotherapy.
It also cannot guarantee that every cell at the edge of the visible ice ball has been destroyed. Incomplete coverage can lead to residual or recurrent disease, making follow-up imaging essential.
AI-controlled freezing, autonomous robotic probe placement, reliable cryo-immunotherapy and patient-specific digital-twin planning remain developmental rather than standard clinical practice.
KEY TAKEAWAY
MRI-guided cryoablation represents a major shift in cancer treatment.
The innovation is not simply the use of extreme cold. It is the ability to combine minimally invasive probe-based treatment with detailed imaging and real-time monitoring.
This approach reflects a broader movement:
From removing large amounts of tissue to targeting selected disease.
From major surgical exposure to image-guided access.
From planning treatment only before the procedure to monitoring it as it happens.
MRI-guided cryoablation is already clinically useful in carefully selected patients, particularly when precise targeting, organ preservation or avoidance of major surgery is important.
Its future may become even more personalised through AI planning, robotic probe placement and patient-specific treatment simulation.
The future of tumour treatment may not always be about opening the body. It may be about seeing the target clearly and destroying it with millimetre-level control.
REFERENCES
- Erinjeri JP, Clark TWI. Cryoablation: mechanism of action and devices. Journal of Vascular and Interventional Radiology. 2010;21(8 Suppl):S187–S191. DOI: https://doi.org/10.1016/j.jvir.2009.12.403
- Baust JG, Gage AA, Bjerklund Johansen TE, Baust JM. Mechanisms of cryoablation: clinical consequences on malignant tumors. Cryobiology. 2014;68(1):1–11. DOI: https://doi.org/10.1016/j.cryobiol.2013.11.001
- Mahnken AH, König AM, Figiel JH. Current technique and application of percutaneous cryotherapy. Rofo. 2018;190(9):836–846. DOI: https://doi.org/10.1055/a-0598-5134
- Ahrar K, Ahrar JU, Javadi S, et al. Real-time magnetic resonance imaging-guided cryoablation of small renal tumors at 1.5 T. Investigative Radiology. 2013;48(6):437–444. DOI: https://doi.org/10.1097/RLI.0b013e31828027c2
- Bhagavatula SK, Tuncali K, Shyn PB, Levesque VM, Chang SL, Silverman SG. Percutaneous CT- and MRI-guided cryoablation of cT1 renal cell carcinoma: intermediate- to long-term outcomes in 307 patients. Radiology. 2020;296(3):687–695. DOI: https://doi.org/10.1148/radiol.2020200149
- Cazzato RL, De Marini P, Leonard-Lorant I, et al. Safety and oncologic outcomes of magnetic resonance imaging-guided cryoablation of renal cell carcinoma: a 10-year single-center experience. Investigative Radiology. 2021;56(3):153–162. DOI: https://doi.org/10.1097/RLI.0000000000000719
- Abdelsalam ME, Mecci N, Awad A, et al. Magnetic-resonance-imaging-guided cryoablation for solitary-biopsy-proven renal cell carcinoma: a tertiary cancer center experience. Cancers. 2024;16(10):1815. DOI: https://doi.org/10.3390/cancers16101815
- Cazzato RL, De Marini P, Mayer T, et al. MRI- versus CT-guided renal tumor cryoablation: is there a difference? Cardiovascular and Interventional Radiology. 2023;46:901–910. DOI: https://doi.org/10.1007/s00270-023-03453-7
- Jennings JW, Prologo JD, Garnon J, et al. Cryoablation for palliation of painful bone metastases: the MOTION multicenter study. Radiology: Imaging Cancer. 2021;3(2):e200101. DOI: https://doi.org/10.1148/rycan.2021200101
- Lee TC, Guenette JP, Moses ZB, Chi JH. MRI-guided cryoablation of epidural malignancies in the spinal canal resulting in neural decompression and regrowth of bone. American Journal of Roentgenology. 2019;212(1):205–208. DOI: https://doi.org/10.2214/AJR.18.19951
- Bodard S, Geevarghese R, Razakamanantsoa L, et al. Percutaneous cryoablation in soft tissue tumor management: an educational review. Insights into Imaging. 2024;15:278. DOI: https://doi.org/10.1186/s13244-024-01822-5
- Fine RE, Gilmore RC, Tomkovich KR, et al. Cryoablation without excision for early-stage breast cancer: ICE3 trial 5-year follow-up on ipsilateral breast tumor recurrence. Annals of Surgical Oncology. 2024;31:7273–7283. DOI: https://doi.org/10.1245/s10434-024-16181-0
- Sidana A, Tayebi S, Blank F, et al. Magnetic resonance imaging-ultrasound fusion guided focal cryoablation for men with intermediate-risk prostate cancer. Urologic Oncology. 2024;42(5):158.e1–158.e10. DOI: https://doi.org/10.1016/j.urolonc.2024.01.003
- Aarts BM, Klompenhouwer EG, Rice SL, et al. Cryoablation and immunotherapy: an overview of evidence on its synergy. Insights into Imaging. 2019;10:53. DOI: https://doi.org/10.1186/s13244-019-0727-5