
Introduction
Medical imaging is already digital, data-rich, and fundamental to routine diagnosis, making radiology one of the most obvious testing grounds for artificial intelligence. Artificial intelligence , or AI , refers to computer systems that can learn patterns from data . In radiology , this commonly includes machine learning and deep learning , where algorithms are trained to discover visual patterns in X-rays , CT scans , MRI scans , ultrasound images , or mammograms . The key difference is not that AI is replacing radiologists, but that it is starting to help with repetitive image processing, triage of urgent cases, reconstruction of scans, screening and reporting. The U.S. Food and Drug Administration (FDA) publishes a public list of AI-enabled medical devices authorized for marketing . A 2025 analysis of FDA-authorized AI/ML devices found that image-based tools remained the predominant category, and radiology as the lead review panel for the majority of imaging-based devices . The word "breakthrough" should be used with caution in medicine. The biggest advancements in radiology AI are not splashy statements that a machine can “see better than doctors” all the time. These are real gains: helping to find breast cancer earlier in screening programmes, warning stroke teams sooner, aiding the assessment of lung nodules, lowering radiation or scan time, and retrieving preventive-health information from scans previously completed. These developments are important because radiology departments are facing increased imaging volumes and workforce shortages, and a clinical imperative to give reliable results fast.
Why Radiology Needed AI: The Pressure Behind the Technology
Radiology is pattern recognition, but the context of that pattern recognition has become more complicated. A CT scan, or computed tomography scan, is when X-rays are taken from many angles to create cross-sectional pictures of the body. MRI, or magnetic resonance imaging, uses magnetic fields and radiofrequency signals to create detailed images of soft tissue. Mammography uses low-dose X-rays to screen for breast cancer. These technologies produce huge amounts of picture data. Each scan may have hundreds or thousands of images that need to be analysed in clinical context. This concerns since a missed finding can delay care, an unneeded false alert can lead to worry, more testing, and cost. Radiology has a process problem, not only a diagnosis problem. Routine cancer staging scans, screening checks and follow-up imaging may be done at the same time as emergency scans for stroke, hemorrhage, pulmonary embolism or trauma. AI-based computer-aided triage sorts or flags important discoveries to alert physicians more quickly, while computer-aided detection identifies worrisome regions for radiologist assessment. FDA-authorized AI-enabled devices have passed appropriate premarket requirements, but authorization does not mean that each tool is going to improve patient outcomes in all hospital environments.
A helpful way to think of radiology AI is as a “second layer” on top of the imaging process. Some technologies evaluate images after capture, some recreate clearer images from raw scan data, some extract metrics such as bone density or coronary calcium, and some process the radiology report itself. A 2025 taxonomy of 1,016 FDA AI/ML authorizations revealed 736 unique devices, of which 621 used images as the primary input. Of imaging-based devices, radiology was the lead review panel for 88.2% of them. It also explains the rapid uptake of AI in radiology compared to a number of other medical fields.
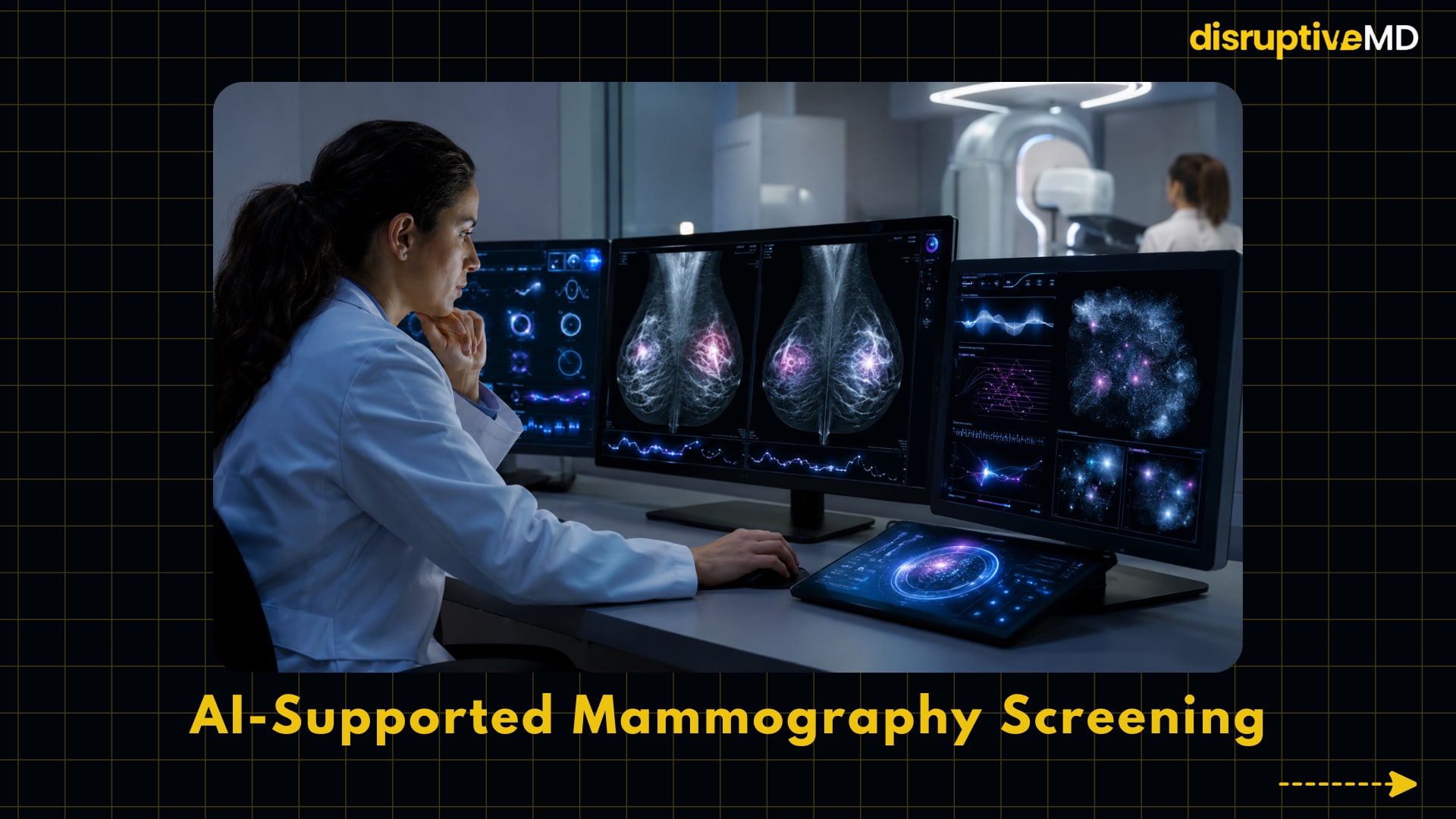

- AI-supported mammography helps flag suspicious breast imaging patterns and can assist radiologists in screening workflows.
- The MASAI trial showed AI-supported screening could reduce reader workload while maintaining careful human radiologist review.
- The key value is not replacing radiologists, but helping screening programs detect important cancers while managing workload pressure.
What the Technology Does: Five Breakthroughs of AI in Radiology
1. AI-supported mammography screening
AI-supported mammography is one of the most compelling examples of radiology AI transitioning from laboratory testing to clinical evidence at the population level. Mammography screening is intended to uncover breast cancer before symptoms develop, but screening programmes must balance sensitivity, the ability to find cancer, with false positives, aberrant results that subsequently reveal not to be disease. AI tools can provide a risk score, flag worrisome areas and help determine if a case should be reviewed by one or two radiologists. The strongest data comes from the MASAI trial, a randomized Swedish mammography screening study of more than 100,000 women. In the AI-supported arm, the system examined mammograms, triaged low risk cases to single reading and higher risk instances to double reading with radiologist support. When full findings were revealed in 2026, there were 1.55 interval cancers per 1,000 women in the AI-supported group against 1.76 per 1,000 women in the standard double-reading group, with equal false-positive rates of 1.5% and 1.4%, respectively. Earlier trial studies also showed a 44% reduction in the workload of screen readers and a 29% increase in cancer diagnosis without increasing false positives. This is critical since mammography screening relies on both accuracy and labour capacity. Interval cancers (malignancies discovered after a negative screen and before the next scheduled test) are of clinical interest as they may be tumors missed at screening or fast-growing cancers. The MASAI statistics are not to suggest that AI should replace radiologists, the trial still needed a human radiologist evaluation. The key breakthrough is that AI may allow screening programmes to detect more clinically important malignancies, while decreasing workload pressure if implementation is accompanied by diligent monitoring and local validation.
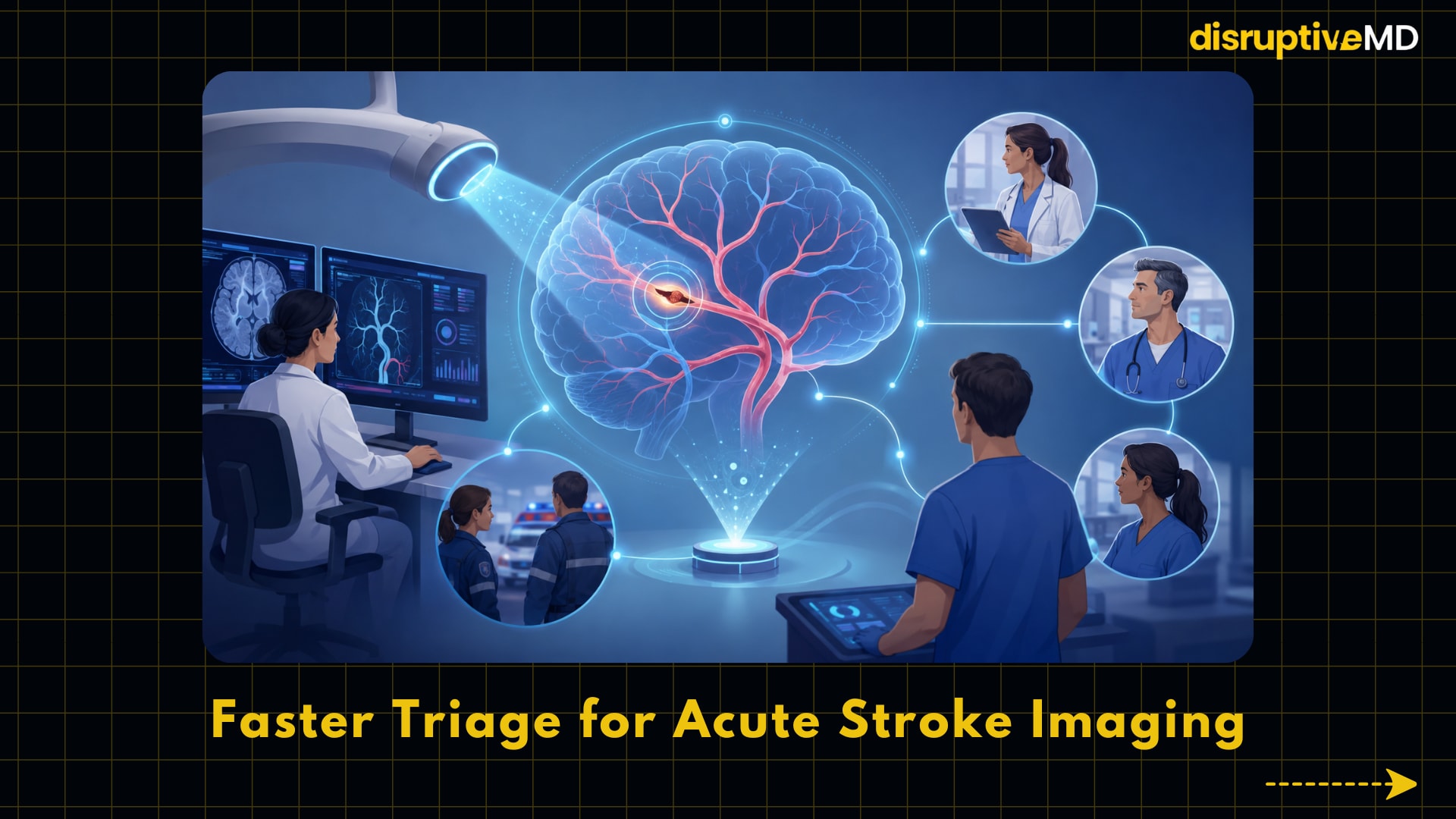
2. Faster triage for acute stroke imaging
AI-enabled stroke triage is a breakthrough since it’s not only about visual interpretation but about time. In the context of an acute ischemic stroke, a large vascular occlusion (LVO) is a major artery providing blood flow to the brain that is blocked by a clot. These patients may be eligible for endovascular thrombectomy, where doctors remove the clot through a catheter, although the benefit is highly time-dependent. CT angiography, a CT scan of the blood vessels, can be analysed by AI techniques that can warn stroke teams when an LVO is detected. A cluster randomized stepped-wedge clinical study in JAMA Neurology evaluated AI-enabled automated LVO identification at four comprehensive stroke centers . Among 243 eligible thrombectomy-treated patients, the use of the AI system was associated with a reduction of 11.2 minutes in door-to-groin time (from hospital arrival to catheter access for thrombectomy) and 9.8 minutes from CT scan to start of endovascular treatment. The study failed to show a statistically significant improvement in functional independence at 90 days, an important reminder that workflow improvements do not necessarily directly translate into quantifiable clinical outcomes. This concerns because stroke care is a team sport involving emergency physicians, radiologists, neurologists, interventional specialists, nurses and transfer systems. AI triage can help reduce communication delays by alerting the appropriate team sooner, but it must be embedded into real hospital procedures. The advance is not in autonomous diagnosis, but in speedier coordination on a time-critical imaging finding.
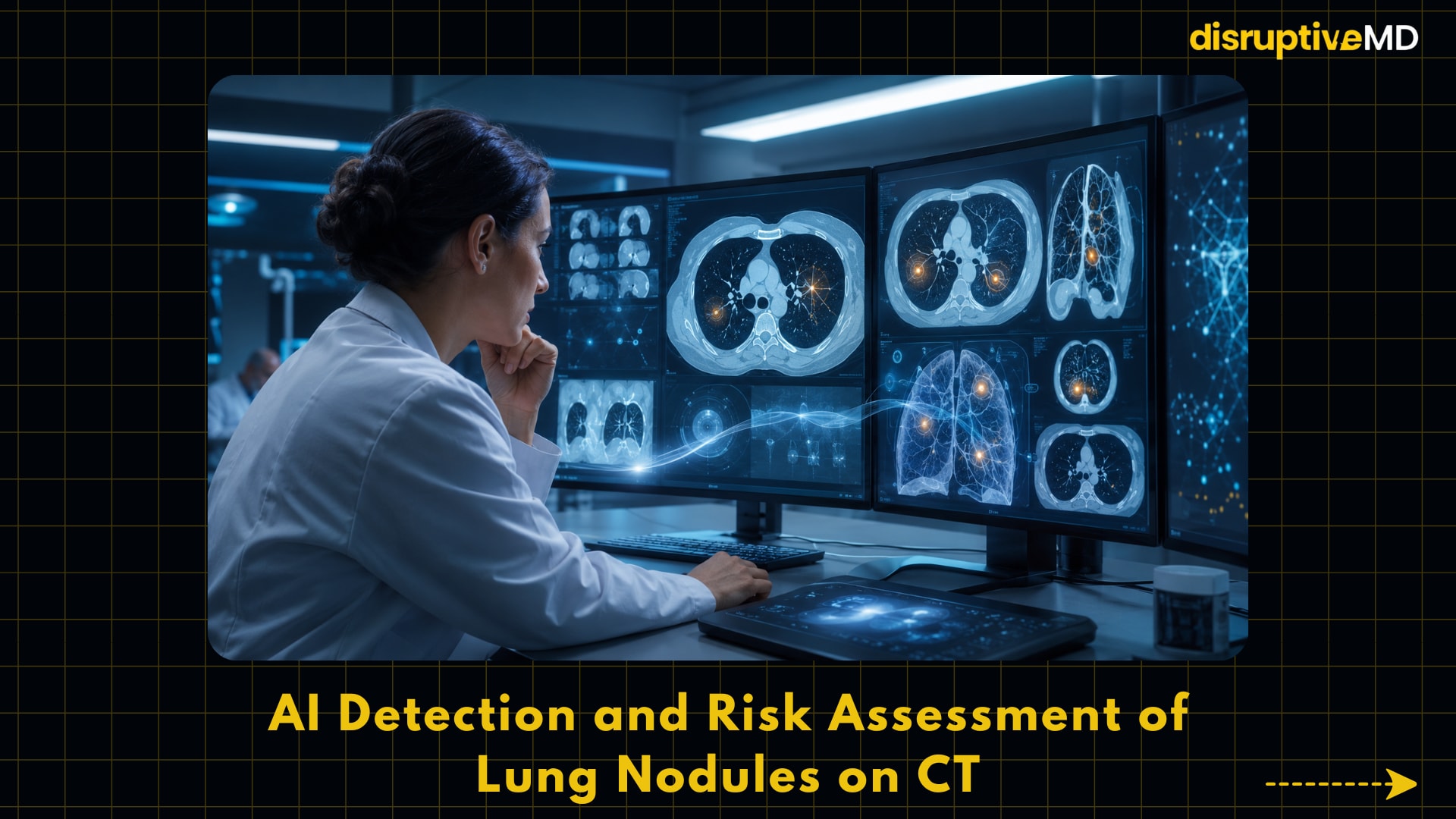
3. AI detection and risk assessment of lung nodules on CT
AI for lung nodule detection tackles one of the most difficult problems in thoracic radiology. A pulmonary nodule is a small area observed in the lung on imaging. Most are benign, but some are early lung cancer. Low-dose CT screening can detect lung cancer earlier in high-risk populations but also provides many results that require cautious interpretation. AI-based computer-aided detection can help with the detection of nodules . AI-based classification models can help to determine whether a nodule is more likely benign or malignant . A 2025 systematic review of AI performance for detecting lung cancer on CT reported 14 studies, seven for detection and eight for classification. The studies analysed for detection showed that the sensitivity of AI models ranged from 86.0% to 98.1%, compared to 68% to 76% for radiologists in the relevant papers, but the specificity was lower for AI at 77.5% to 87%, compared to 87% to 91.7% for radiologists. Sensitivity refers to the ability to detect disease and specificity refers to the ability to distinguish non-disease; there is a trade-off here in that a highly sensitive technology will also detect more benign findings. This is important, as lung cancer screening programs can increase imaging volume and require consistent nodule follow-up. AI can help radiologists avoid missing nodules and normalize measures over time, but false positives can lead to more surveillance scans and biopsies and patient concern. The actual breakthrough is not a stand-alone cancer diagnosis, but consistency with AI assistance.
4. Deep-learning reconstruction for lower-dose CT and faster MRI
Some of the most useful radiology AI doesn’t diagnose anything, it improves how images are made. Image reconstruction is the process of turning the raw data from the scanner into images that clinicians can analyse. Older CT reconstruction algorithms, such as filtered back projection, are computationally quick but may yield noisy images at low radiation doses. Model-based iterative reconstruction can enhance image quality but may be slower or produce odd image texture. Deep-learning reconstruction use AI models trained on imaging data to produce higher quality images from lower dose or under sampled data. While deep-learning reconstruction may generate high-quality CT images from lower-dose data more rapidly than some model-based iterative techniques, performance varies significantly based on training data and scanner context, according to a review in Radiology. In MRI A prospective clinical investigation in knee MRI showed that deep-learning reconstruction allowed for an almost twofold reduction in scan time while being diagnostically equal to a conventional procedure in 170 patients, whose exams were reviewed by six musculoskeletal radiologists . This is important because scan time, radiation dose and image quality are practical hurdles in healthcare. Faster MRI can help reduce patient discomfort, motion artifacts and waiting waits. CT reconstruction for lower-dose scans enables safer repeat scans, especially in the follow-up or screening setting. The major restriction is that reconstruction AI has to be properly evaluated so that it does not smooth subtle illness or create misleading image appearances.
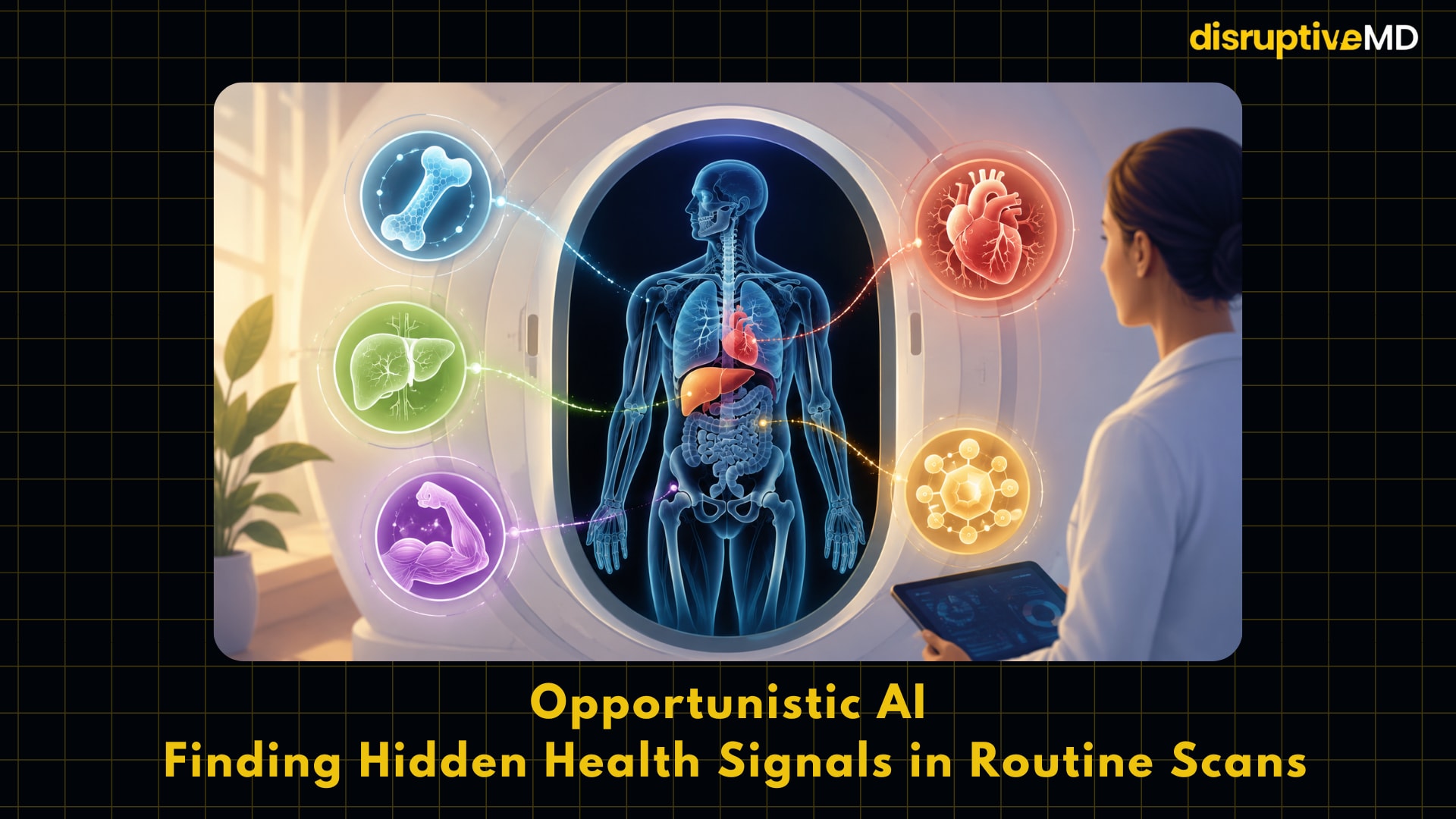
5. Opportunistic AI: finding hidden health signals in routine scans
Opportunistic AI is a more recent radiology development that alters what a scan can provide. Opportunistic screening is the utilization of imaging performed for another purpose to obtain useful health information. For instance, a chest or abdominal CT performed for discomfort, cancer staging, or lung screening can also give information on bone density, coronary artery calcium, fatty liver, skeletal muscle, or visceral fat. AI could automate these measures and help translate “incidental” imaging data into preventive-health signals. Clinically the appeal is considerable as no additional scan, radiation exposure or patient appointment is necessary. A 2026 review in Radiology describes opportunistic CT screening for unsuspected or presymptomatic conditions such as osteoporosis, cardiovascular disease, sarcopenia, and hepatic steatosis. Explainable AI tools can quantify body composition measures and generate quality-assurance images for radiologist verification. One validation study showed that an FDA-approved AI-enabled tool for bone mineral density measurement in coronary artery calcium scans accurately identified osteoporosis and osteopenia with findings comparable to manual measures. This is important because radiology might be used more and more in prevention, and not merely diagnosis. A CT scan performed for one clinical inquiry may detect silent fracture risk, metabolic risk, or cardiovascular risk that would otherwise be overlooked. The breakthrough is wider use of existing imaging data, but the implementation problem is huge: health systems must decide who acts on these results, how they are reported, how false positives are handled, and whether patients get proper follow-up.
Evidence and Real-World Meaning
The strongest current evidence for radiology AI is uneven across use cases. AI-supported mammography has become part of the domain of randomized trial evidence, with the MASAI study showing improved screening performance without an increased false-positive rate in the scenario investigated. Stroke triage has evidence for randomized workflow with faster treatment times but improvement in long-term impairment results were not clearly shown in the mentioned experiment. Systematic-review evidence supports the detection performance of lung CT AI, although specificity and false-positive treatment remain relevant problems. Deep-learning reconstruction offers a strong technical and emerging clinical evidence, especially for picture quality and scan acceleration. There is encouraging validation evidence for opportunistic AI, but many applications still require outcome studies to demonstrate that the automated identification translates to improved prevention and treatment. In real-world healthcare, the question isn’t whether AI does well on a test dataset, it’s if it improves judgments. It may be beneficial if a model finds more nodules, capturing early cancer, but it may be harmful to efficiency if it generates numerous unwarranted recalls. A stroke alert can save time if the team responds effectively and trusts the signal, but can lead to alert fatigue if it frequently results in false alarms. A reconstruction model might save scan time but tiny abnormalities have to be preserved. This is the reason that radiology AI requires clinical validation, workflow design, post-deployment monitoring and radiologist oversight. The regulatory approval is a good thing, but it should not be confused with a universal clinical validation.” The FDA list enhances openness by specifying the AI-enabled devices that have been cleared or approved for marketing and the FDA states that listed devices have met applicable premarket requirements for safety and effectiveness. However, performance may vary according on scanner, imaging protocol, patient group, disease prevalence, and clinical workflow.
Limitations, Risks, and Unanswered Questions
The biggest restriction of AI in radiology is generalizability. A model trained on pictures acquired from a different region, scanner type or patient group, may not perform as well when applied in a different scenario. This is particularly relevant for global healthcare when imaging equipment, disease patterns, body habitus, ethnicity and availability to follow-up care differ greatly. The World Health Organization has stressed that AI in health should have ethics and human rights at the centre of design, deployment and governance, including consideration of accountability and public benefit. Bias is another issue. AI tools may not be as reliable for certain demographics if the training data are not representative of those communities. The authors emphasized that race and ethnicity data were not obtained in the MASAI trial and that the study was conducted in one country with one AI system and one type of mammography device, which may restrict generalizability. This is not to downplay the trial’s value, but it does illustrate why wider validation is needed before assuming the same results across other countries and screening systems. There are also safety concerns about automation bias, when clinicians over-trust a computer generated output. A radiologist may overlook a finding if an AI tool fails to identify it; or, a radiologist may overcall a benign anomaly if AI highlights it too forcefully. The World Health Organization (WHO) has emphasized that generative AI and massive multimodal models that can produce text, summary or image-related outputs have yet to prove their ability to safely perform every therapeutic duty. Cost and implementation to be determined. AI software may include license fees, integration with picture archiving and communication systems, cybersecurity review, clinical training, quality assurance and legal governance. For health systems with limited resources, the most helpful AI may not be the most technically spectacular model, but the tool that reliably addresses a high-volume clinical problem at acceptable cost.
Conclusion
Artificial intelligence in radiology is becoming therapeutically relevant, but its most crucial purpose is to assist, not replace. The top five best-developed domains include AI-supported mammography screening, acute stroke triage, lung nodule identification, deep-learning image reconstruction, and opportunistic extraction of preventive-health biomarkers from regular scans . Each one offers a distinct type of value: earlier detection, faster care, more consistent measurement, safer or faster imaging, and wider use of current data. The future of radiology AI will be less about headline-grabbing accuracy promises, and more on careful implementation. Useful AI requires validation in broad populations, post-deployment monitoring, integration into clinical workflows, and governance by doctors knowledgeable about both medicine and the limitations of algorithms. The promise for patients and health systems is not a fully automated radiology department. The realistic promise is a radiological service that’s faster, more consistent, more quantitative and better integrated to preventative and emergency care.
Evidence Rating
Mixed or limited evidence. AI in radiology offers FDA-approved tools and some robust clinical trial findings, particularly in mammography screening and stroke process triage. However, other applications including lung nodule classification, opportunistic screening, reconstruction in all body areas, and generative reporting tools still need wider external validation, outcome studies, subgroup analysis, cost effectiveness research, and continuous monitoring in routine clinical practice.
Educational Disclaimer
This material is for informational purposes only and is not a substitute for professional medical advice, diagnosis or treatment. Decisions about medical imaging should be made by qualified doctors on the basis of the individual patient, clinical context and locally established standards of care.
References
- U.S. Food and Drug Administration. Artificial Intelligence-Enabled Medical Devices.
- Singh, R., Bapna, M., Diab, A.R. et al. How AI is used in FDA-authorized medical devices: a taxonomy across 1,016 authorizations. npj Digit. Med. 8, 388 (2025). https://doi.org/10.1038/s41746-025-01800-1.
- Gommers J, Hernström V, Josefsson V et al. Interval cancer, sensitivity, and specificity comparing AI-supported mammography screening with standard double reading without AI in the MASAI study: a randomised, controlled, non-inferiority, single-blinded, population-based, screening-accuracy trial, The Lancet, 407, 505-514.
- Martinez-Gutierrez JC, Kim Y, Salazar-Marioni S, et al. Automated Large Vessel Occlusion Detection Software and Thrombectomy Treatment Times: A Cluster Randomized Clinical Trial. JAMA Neurol.2023;80(11):1182–1190. doi:10.1001/jamaneurol.2023.3206.
- Cheo HM, Ong CYG, Ting Y. A Systematic Review of AI Performance in Lung Cancer Detection on CT Thorax. Healthcare (Basel). 2025 Jun 24;13(13):1510. doi: 10.3390/healthcare13131510. PMID: 40648536; PMCID: PMC12250385.
- Koetzier LR, et al. Deep Learning Image Reconstruction for CT: Technical Principles and Clinical Prospects.Radiology, 2023.
- Johnson PM, et al. Deep Learning Reconstruction Enables Prospectively Accelerated Clinical Knee MRI.Radiology, 2023.
- Pickhardt PJ, et al. CT-based Opportunistic Screening for Adding Clinical Value. Radiology, 2026.
- Naghavi M, et al. Validation of Opportunistic Artificial Intelligence-Based Bone Mineral Density Measurements in Coronary Artery Calcium Scans. 2024.
- World Health Organization. Ethics and governance of artificial intelligence for health. 2021.