
Introduction
Fitness is often discussed through visible changes such as body weight, muscle size, speed, or endurance. But one of the most important signs of fitness is less visible: how well the body can use oxygen when physical demand increases. This is where VO₂ max becomes important.
VO₂ max is widely considered one of the best measurements of cardiorespiratory fitness. It reflects how efficiently the lungs take in oxygen, how effectively the heart and blood deliver it, and how well the muscles use it to produce energy during exercise. In sports, it helps describe aerobic performance potential. In medicine, it can provide useful information about functional capacity, exercise tolerance, and long-term health risk.
The phrase “the new vital sign of fitness” does not mean VO₂ max replaces traditional medical vital signs such as blood pressure, pulse, temperature, respiratory rate, or oxygen saturation. Instead, it means that cardiorespiratory fitness is increasingly recognized as an important health marker that deserves more attention. A person may appear healthy at rest, but their response to exercise can reveal how resilient their heart, lungs, circulation, and muscles really are.
This article explains what VO₂ max is: how it is measured, where it is used, what the evidence supports, what the limitations are, and what readers should realistically understand before treating it as a personal fitness or health number.



- Fitness is often discussed through visible changes such as body weight, muscle size, speed, or endurance.
- But one of the most important signs of fitness is less visible: how well the body can use oxygen when physical demand increases.
- VO₂ max is widely considered one of the best measurements of cardiorespiratory fitness.
What Is VO₂ MAX?
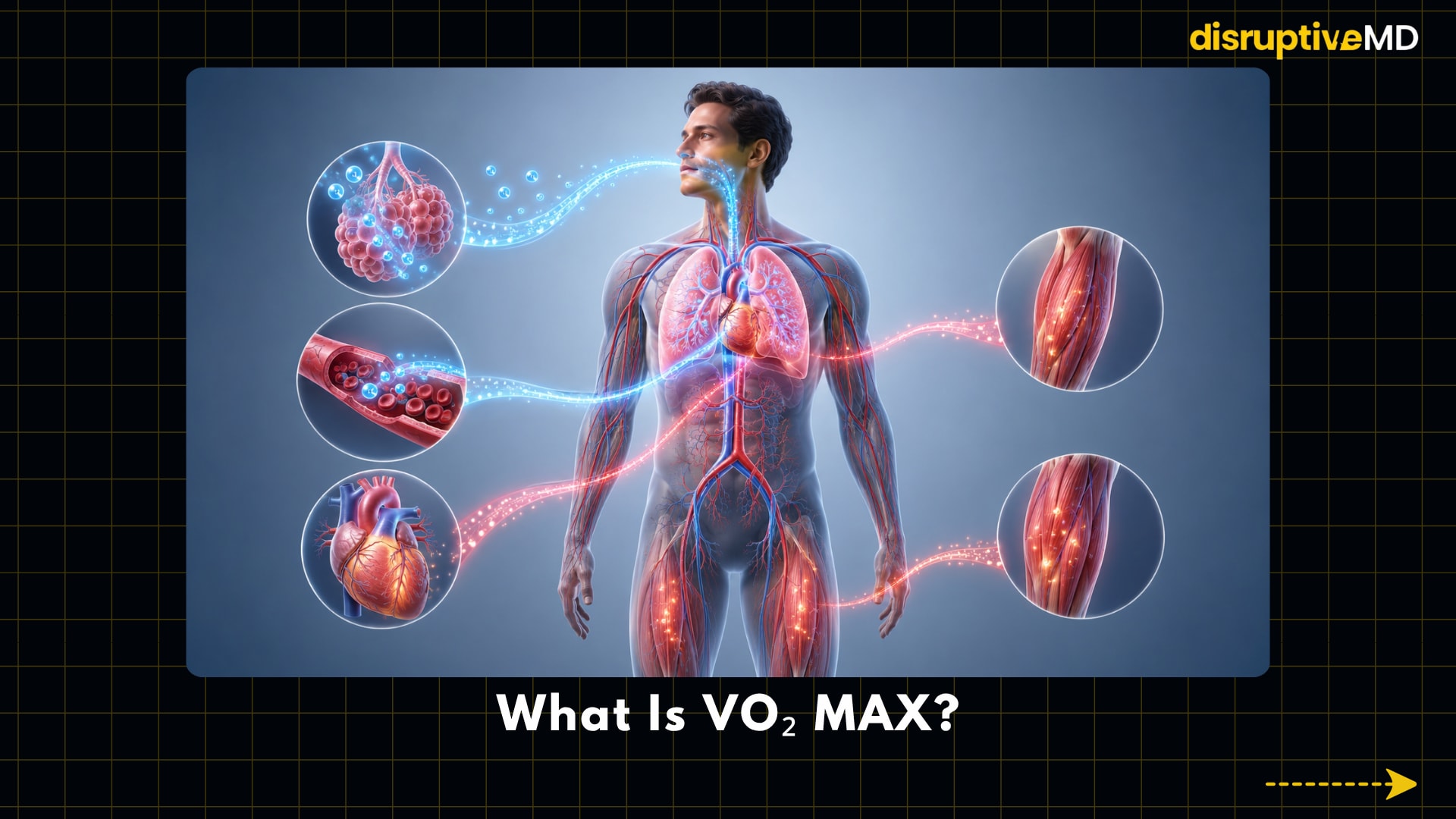
VO₂ max, also called maximal oxygen uptake, is the highest amount of oxygen the body can use during intense exercise. It is usually measured in millilitres of oxygen per kilogram of body weight per minute, written as mL/kg/min.
In simple terms, VO₂ max shows how well the body can take oxygen from the air, move it through the lungs and blood, deliver it through the heart and circulation, and use it inside working muscles to produce energy. It is not only a “lung number” or a “fitness score.” It reflects the combined performance of the lungs, heart, blood, blood vessels, muscles, and cellular energy systems. A higher VO₂ max generally means the body can support more intense aerobic activity before fatigue becomes limiting. This is why VO₂ max is widely used in exercise science, sports medicine, cardiology, pulmonary medicine, and rehabilitation.
However, VO₂ max should not be misunderstood as the only marker of fitness. Strength, mobility, body composition, movement skill, recovery, sleep, metabolic health, and injury risk also matter. VO₂ max is best understood as one important measurement of cardiorespiratory fitness, not a complete picture of health.
In clinical testing, the term “peak VO₂” is often used instead of true VO₂ max. This is because some people, especially patients with heart or lung disease, may stop exercise because of symptoms before reaching a clear physiological maximum. Peak VO₂ is the highest oxygen uptake recorded during that test, while true VO₂ max usually requires evidence that oxygen uptake has plateaued despite increasing exercise intensity.
How Is It Measured?
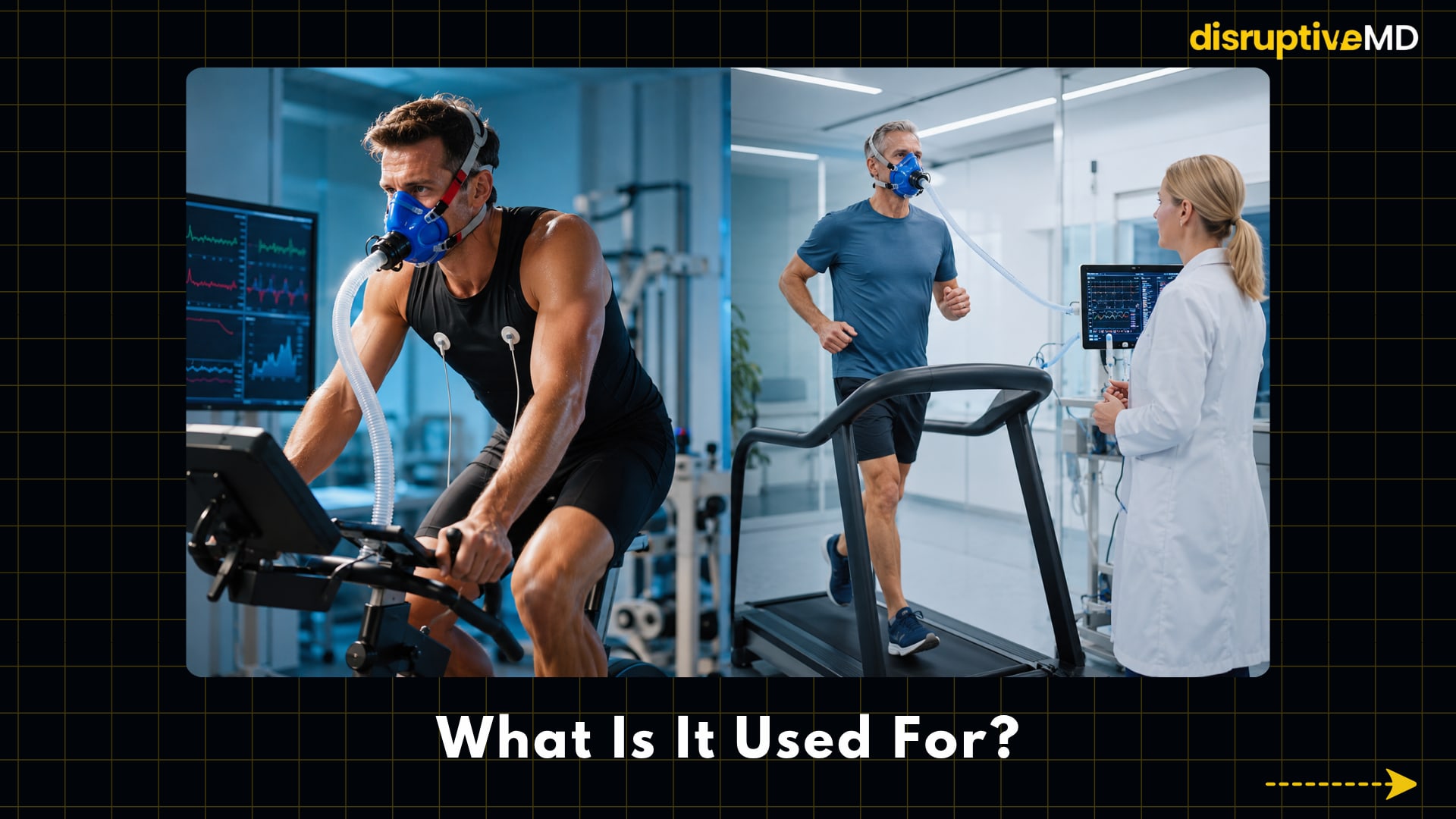
The most accurate way to measure VO₂ max is through cardiopulmonary exercise testing, often called CPET. During CPET, a person exercises on a treadmill or stationary cycle while wearing a mask or mouthpiece connected to equipment that measures oxygen use, carbon dioxide production, breathing, and ventilation. Heart rate, blood pressure, symptoms, and sometimes ECG rhythm are also monitored.
The test usually becomes progressively harder until the person reaches maximal effort or stops because of fatigue, breathlessness, chest discomfort, leg fatigue, or another clinical reason. The final value is interpreted by trained professionals, especially when the test is being done for medical reasons.
VO₂ max can also be estimated rather than directly measured. Common estimation methods include treadmill protocols, cycle ergometer tests, step tests, field running tests, walking tests, and wearable-device algorithms. These estimates can be useful for general tracking, fitness coaching, or population screening, but they are not the same as directly measured VO₂ max from laboratory-grade gas analysis.
Wearables may estimate VO₂ max using heart rate, pace, movement data, age, sex, body size, and proprietary algorithms. These estimates can be helpful for trends over time, but they may be inaccurate in individuals, especially when the algorithm is not validated for that person’s age, disease status, sport, medication use, or fitness level.
The quality of VO₂ max measurement depends on several factors: proper equipment calibration, the exercise protocol used, whether the person gave maximal effort, the type of exercise used, the person’s familiarity with the test, hydration, sleep, recent training, altitude, medication, and medical conditions.
What Is It Used For?
VO₂ max is used to assess cardiorespiratory fitness, which means the ability of the heart, lungs, blood, and muscles to support sustained physical activity.
In fitness and sports, it is used to evaluate aerobic capacity, monitor training progress, compare endurance potential, design training zones, and assess how the body responds to structured exercise. Endurance athletes such as runners, cyclists, swimmers, rowers, and football players may use VO₂ max as one marker of performance capacity.
In medicine, VO₂ max or peak VO₂ can help assess functional capacity. Functional capacity means how much physical work a person can safely perform. This can be relevant in heart failure, pulmonary disease, unexplained breathlessness, cardiac rehabilitation, pulmonary rehabilitation, pre-operative assessment, and recovery after illness.
In research, VO₂ max is often used as an outcome measure in studies of exercise training, cardiovascular disease, obesity, ageing, rehabilitation, metabolic health, and athletic performance. Researchers may use it to understand whether an intervention improves aerobic fitness.
VO₂ max is also used in risk assessment. Low cardiorespiratory fitness has been associated with higher risk of cardiovascular disease and all-cause mortality in large observational studies. This does not mean VO₂ max alone diagnoses disease, but it can add meaningful information about long-term health risk.
Why Is It Significant?
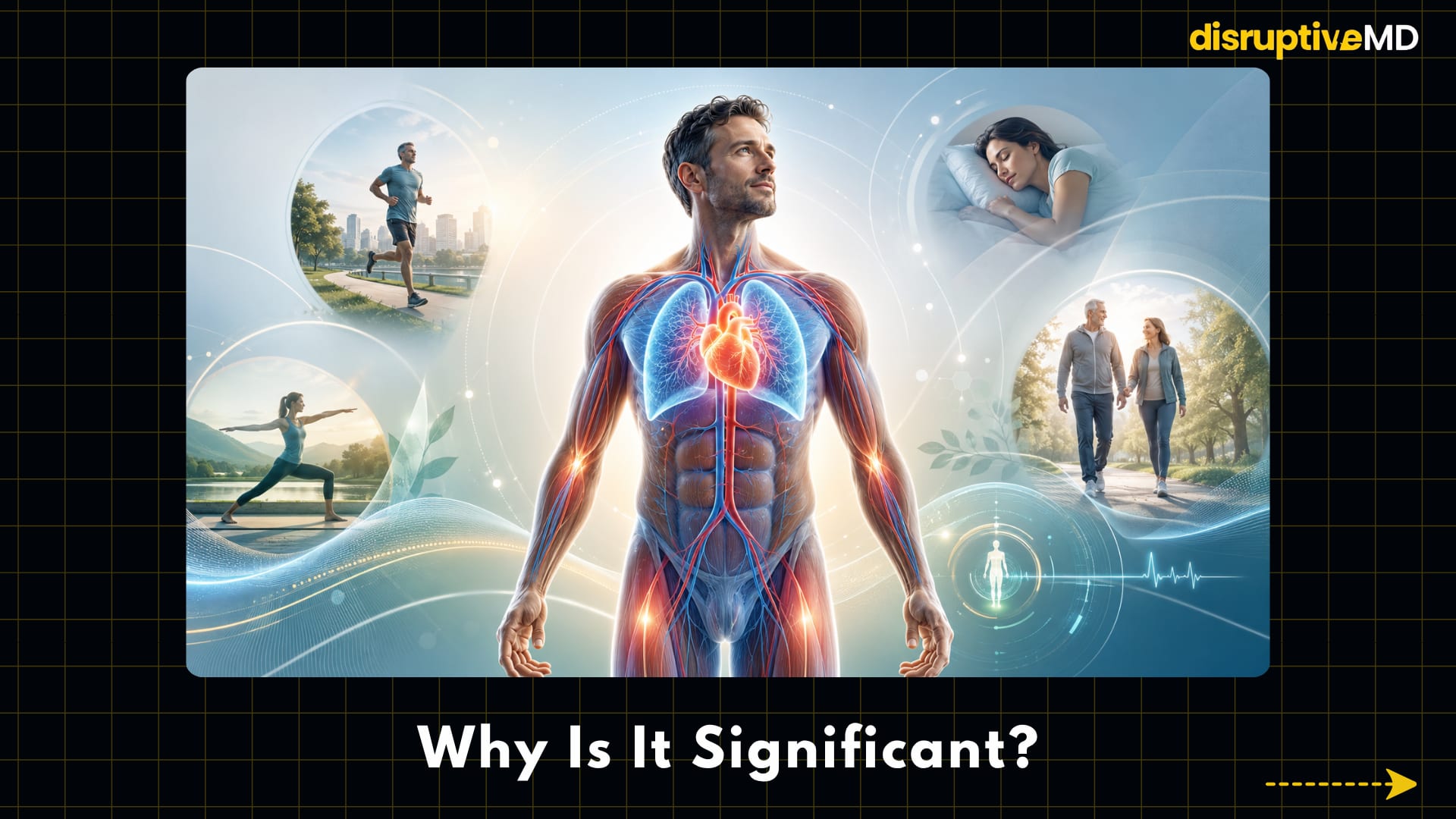
VO₂ max is significant because it turns fitness into an objective physiological measurement. Instead of simply asking whether someone is “fit,” VO₂ max gives a measurable estimate of how well the body performs during increasing physical stress.
The American Heart Association has argued that cardiorespiratory fitness should be treated as a clinical vital sign because it provides important information about health risk. This does not mean VO₂ max has officially replaced traditional vital signs such as blood pressure, pulse, respiratory rate, temperature, or oxygen saturation. Instead, it means cardiorespiratory fitness may deserve more routine attention in healthcare because it reflects a person’s physiological reserve.
Physiological reserve means the body’s ability to tolerate stress. A person with higher cardiorespiratory fitness may have more reserve during exercise, illness, surgery, rehabilitation, or daily physical demands. A person with exceptionally low fitness may become breathless or fatigued at lower workloads, even if resting measurements appear normal.
VO₂ max is also significant because it is modifiable. Genetics, age, sex, body size, disease, and training history influence VO₂ max, but structured aerobic training can improve cardiorespiratory fitness in many people. This makes VO₂ max different from many static risk factors. It can be measured, monitored, and improved.
For athletes, VO₂ max can help explain endurance potential. For clinicians, it can help reveal how the heart, lungs, circulation, and muscles respond under stress. For general readers, it is a reminder that fitness is not only about appearance or body weight; it is also about how efficiently the body produces energy during movement.
Is It Approved, Commonly Used, Research-Stage, or Experimental?
VO₂ max itself is not a drug, procedure, implant, or therapy, so it is not “approved” in the same way a medication or medical device is approved. It is a physiological measurement.
Direct VO₂ measurement through CPET is an accepted and commonly used method in exercise physiology, sports performance, cardiology, pulmonary medicine, and rehabilitation. In clinical settings, CPET equipment and gas-analysis systems may fall under medical-device regulation, depending on the country and device type. For example, oxygen uptake computers and respiratory gas analyzers are regulated device categories in the United States.
VO₂ max testing is commonly used in sports science and performance testing. In medicine, CPET is well established but not used as routinely as blood pressure, ECG, or basic laboratory tests because it requires specialized equipment, trained staff, time, patient effort, and safety protocols.
Estimated VO₂ max from equations, field tests, or wearables is commonly used in fitness settings, but its clinical role is more limited. These estimates should not be treated as diagnostic results unless the method and device have been validated for that clinical purpose.
Wearable-based VO₂ max estimation is an active area of research and consumer health tracking. It is not experimental in the sense that many devices already provide estimates, but its medical use remains more uncertain than laboratory CPET. A smartwatch estimate may encourage fitness awareness, but it should not be used alone to diagnose heart disease, lung disease, or training readiness.
How Is It Used in Real Clinical Practice or Research?
In real clinical practice, VO₂ max or peak VO₂ is most often measured through CPET when clinicians need a more detailed understanding of exercise limitation. This may be useful when symptoms such as breathlessness, exercise intolerance, fatigue, or poor functional capacity are not fully explained by resting tests.
In cardiology, CPET can help evaluate patients with heart failure, assess prognosis, guide rehabilitation, and contribute to advanced heart failure or transplant evaluation. Importantly, peak VO₂ is not used alone to make major clinical decisions. It is interpreted with symptoms, imaging, blood tests, ECG findings, ventilatory efficiency, medication status, comorbidities, and overall clinical judgment. I n pulmonary medicine, CPET can help distinguish whether exercise limitation is more likely related to lung disease, heart disease, poor conditioning, abnormal breathing response, circulatory limitation, or mixed causes. This can be especially useful when resting lung function tests do not fully explain the patient’s symptoms.
In rehabilitation, VO₂ max or related CPET data can help prescribe safe exercise intensity, track improvement, and document recovery. In cardiac rehabilitation and pulmonary rehabilitation, the goal is not simply to increase a number but to improve function, safety, confidence, and daily-life capacity.
In research, VO₂ max is used as a measurable endpoint. Studies may examine whether exercise training, rehabilitation, weight-loss interventions, medications, ageing-related interventions, or disease-management programs improve aerobic capacity. Researchers also use VO₂ max or estimated cardiorespiratory fitness to study long-term associations with mortality, cardiovascular disease, metabolic health, cancer outcomes, brain health, and healthcare costs.
Role in Fitness, Sports Performance, Health, or Medicine
VO₂ max plays an important role in fitness because it reflects the body’s ability to produce energy aerobically during sustained activity. Aerobic energy production means using oxygen to help convert fuel into usable energy. This matters for activities such as running, cycling, swimming, hiking, football, tennis, combat sports, and even daily tasks like climbing stairs.
In sports performance, VO₂ max is one important marker of endurance potential. Athletes with a high VO₂ max can usually sustain higher aerobic workloads. However, VO₂ max does not determine performance by itself. Two athletes with similar VO₂ max values may perform differently because of lactate threshold, movement economy, technique, strength, pacing, heat tolerance, nutrition, recovery, psychology, and injury history.
In general health, VO₂ max is useful because it reflects cardiorespiratory fitness, a strong marker of functional health. Higher fitness is generally associated with better exercise tolerance and lower long-term health risk. Low fitness can identify people who may benefit from structured physical activity, medical evaluation, or rehabilitation.
In medicine, VO₂ max helps move assessment beyond resting measurements. Many health problems become more obvious when the body is stressed by exercise. A person may have normal resting oxygen saturation or resting heart rate but still have abnormal exercise tolerance. CPET can reveal patterns that are not visible at rest.
For people trying to improve health, VO₂ max should be viewed as a guide, not a judgment. A low value does not mean failure. It may reflect inactivity, ageing, illness, medication, obesity, anaemia, poor sleep, recent infection, or lack of training. The practical question is not only “What is my VO₂ max?” but “Can I improve my cardiorespiratory fitness safely over time?”
Risks or Limitations
Direct VO₂ max testing requires intense exercise. For healthy people, this is usually safe when performed properly, but it is still physically demanding. For people with heart disease, lung disease, chest pain, fainting, uncontrolled blood pressure, significant arrhythmias, severe anaemia, recent illness, or unexplained symptoms, testing should be medically supervised or postponed until appropriate evaluation is completed.
Possible risks during maximal exercise testing include dizziness, excessive breathlessness, chest discomfort, abnormal blood pressure response, abnormal heart rhythm, falls, musculoskeletal strain, and rarely serious cardiac events. This is why clinical CPET requires screening, trained supervision, emergency protocols, and appropriate monitoring.
VO₂ max also has interpretation limitations. It is influenced by age, sex, body size, body composition, genetics, training history, altitude, haemoglobin level, medication use, exercise mode, motivation, and test protocol. A treadmill test may produce a different value from a cycle test. A person unfamiliar with cycling may stop because of leg fatigue before reaching true cardiorespiratory maximum.
Weight-relative VO₂ max, expressed as mL/kg/min, can also be misleading in some cases. Because body weight is part of the equation, changes in weight can affect the number even if absolute oxygen use has not changed much. In people with obesity, very low body weight, high muscle mass, or major body-composition changes, interpretation requires caution.
Estimated VO₂ max has additional limitations. Field tests and wearables use prediction equations, not direct gas exchange. They may be useful for broad tracking but can overestimate or underestimate true VO₂ max. A wearable estimate should not be treated as a medical diagnosis, especially when symptoms are present.
Another limitation is that VO₂ max does not measure everything that matters. It does not directly measure strength, flexibility, balance, joint health, sport skill, mental resilience, nutrition, sleep, or recovery. A complete fitness or health assessment should include more than VO₂ max.
Evidence
The evidence supporting VO₂ max and cardiorespiratory fitness is strong, but it is important to understand what kind of evidence exists.
First, there is physiological evidence. CPET directly measures how oxygen uptake, carbon dioxide output, ventilation, heart rate, and exercise workload change during increasing exercise. This makes VO₂ max or peak VO₂ a practical measurement of integrated heart-lung-muscle function.
Second, there are major scientific statements and clinical recommendations. The American Heart Association’s scientific statement on cardiorespiratory fitness argued that fitness should be considered a clinical vital sign because it adds meaningful health-risk information beyond many traditional risk factors. A later update reinforced the importance of assessing cardiorespiratory fitness in healthcare and public health.
Third, there is epidemiological evidence. Large cohort studies and meta-analyses have found that lower cardiorespiratory fitness is associated with higher risk of all-cause mortality and cardiovascular events. A major JAMA meta-analysis reported a graded relationship between cardiorespiratory fitness and future health outcomes. This type of evidence is observational, meaning it shows strong associations but does not prove every part of causality by itself.
Fourth, there is clinical-practice evidence. CPET is used in heart failure, pulmonary disease, rehabilitation, unexplained dyspnoea, and pre-operative assessment because it can provide information that resting tests cannot. Professional statements and guidelines describe its value when performed and interpreted correctly.
Fifth, there is exercise-training evidence. Exercise guidelines and position statements support structured aerobic activity as a method for improving cardiorespiratory fitness in many adults. This does not mean every person responds the same way, but it supports the principle that cardiorespiratory fitness is trainable.
Overall, the evidence does not support using VO₂ max as a magic number or a standalone diagnosis. It supports VO₂ max as a meaningful, measurable marker of cardiorespiratory fitness with important links to performance, function, and health risk.
Evidence Gaps or Doubts
One evidence gap is that much of the long-term health-risk evidence is observational. People with higher cardiorespiratory fitness often differ from people with lower fitness in many ways, including physical activity, smoking status, body composition, diet, socioeconomic factors, medication use, and underlying disease. Researchers adjust for many of these factors, but observational studies cannot remove every possible confounder.
Another uncertainty is how best to implement VO₂ max or cardiorespiratory fitness measurement in routine healthcare. CPET is accurate and informative, but it is not practical for every clinic visit. It requires equipment, trained staff, time, cost, and patient effort. This creates a gap between the scientific value of VO₂ max and its everyday accessibility.
Wearable-based VO₂ max estimation is promising but still imperfect. Different devices use different algorithms, and accuracy can vary depending on the person and the activity data available. Many wearable estimates are better suited for tracking trends in generally healthy users than for diagnosing disease or making major clinical decisions.
There are also questions about standardization. VO₂ max values depend on protocol, exercise mode, calibration, criteria for maximal effort, and whether the result is reported as true VO₂ max or peak VO₂. Without standard testing conditions, comparisons between people or across testing centres can be misleading.
Another gap is that VO₂ max does not capture the full complexity of fitness. A person may have a moderate VO₂ max but excellent strength, mobility, balance, and metabolic health. Another person may have a high VO₂ max but poor recovery, overtraining, low energy availability, injury risk, or unhealthy behaviours. Fitness should be interpreted as a multidimensional concept.
Finally, disease-specific thresholds should not be applied casually to the general population. For example, peak VO₂ values used in advanced heart failure or transplant evaluation have a specific clinical context. They should not be used to frighten healthy people or to make medical conclusions outside that context.
Key Takeaway
VO₂ max is one of the most useful measurements of cardiorespiratory fitness. It shows how well the body uses oxygen during intense exercise and reflects the combined function of the heart, lungs, circulation, blood, muscles, and cellular energy systems.
The phrase “new vital sign of fitness” is useful, but it should be interpreted carefully. VO₂ max is not a replacement for medical vital signs, and it is not a diagnosis by itself. It is a powerful fitness and risk marker that deserves more attention because low cardiorespiratory fitness is strongly linked with poorer health outcomes.
The most accurate way to measure VO₂ max is direct cardiopulmonary exercise testing with gas analysis. Wearables, field tests, and equations can estimate VO₂ max, but estimates should be treated as approximations. They are most useful for tracking broad trends, not for making clinical decisions alone.
For athletes, VO₂ max helps describe aerobic potential, but performance depends on many other factors. For clinicians, peak VO₂ can help assess functional capacity and disease severity in selected patients. For general readers, VO₂ max is a reminder that fitness is not just appearance, weight, or gym strength. It is also the body’s ability to deliver and use oxygen when demand rises.
The practical takeaway is simple: VO₂ max is worth knowing, but it should be interpreted in context. A low value can be improved in many people through safe, progressive aerobic training. A high value is useful but does not guarantee complete health. The goal is not to chase a number blindly. The goal is to build a stronger, more resilient cardiorespiratory system over time.
References
- Nicolas J. Pillon, Joaquin Ortiz de Zevallos, Juleen R. Zierath, Barbara E. Ainsworth, Human development and gender inequality are associated with cardiorespiratory fitness: A global systematic review of V̇O2peak, Journal of Sport and Health Science, 15, (101098), (2026).https://doi.org/10.1016/j.jshs.2025.101098
- Robert Ross, Ross Arena, Jonathan Myers, Peter Kokkinos, Leonard A. Kaminsky, Update to the 2016 American Heart Association cardiorespiratory fitness statement, Progress in Cardiovascular Diseases, Volume 83, 2024, Pages 10-15, ISSN 0033-0620, https://doi.org/10.1016/j.pcad.2024.02.003.
- ATS/ACCP Statement on Cardiopulmonary Exercise Testing, American Journal of Respiratory and Critical Care Medicine, Volume 167, Issue 2, January 2003, Pages 211–277, https://doi.org/10.1164/rccm.167.2.211.
- Austin C. Hogwood, Krzysztof Smarż, Michele Golino, et al. Determinants of cardiorespiratory fitness after successfully reperfused ST-elevation myocardial infarction, Current Problems in CardiologY. (2026).https://doi.org/10.1016/j.cpcardiol.2026.103382
- Kodama S, Saito K, Tanaka S, et al. Cardiorespiratory Fitness as a Quantitative Predictor of All-Cause Mortality and Cardiovascular Events in Healthy Men and Women: A Meta-analysis. JAMA. 2009;301(19):2024–2035. doi:10.1001/jama.2009.681.
- Garber, Carol Ewing Ph.D., FACSM, (Chair); Blissmer, Bryan Ph.D.; Deschenes, Michael R. PhD, FACSM; Franklin, Barry A. Ph.D., FACSM; Lamonte, Michael J. Ph.D., FACSM; Lee, I-Min M.D., Sc.D., FACSM; Nieman, David C. Ph.D., FACSM; Swain, David P. Ph.D., FACSM. Quantity and Quality of Exercise for Developing and Maintaining Cardiorespiratory, Musculoskeletal, and Neuromotor Fitness in Apparently Healthy Adults: Guidance for Prescribing Exercise. Medicine & Science in Sports & Exercise 43(7):p 1334-1359, July 2011. | DOI: 10.1249/MSS.0b013e318213fefb.
- Molina-Garcia, P., Notbohm, H.L., Schumann, M. et al. Validity of Estimating the Maximal Oxygen Consumption by Consumer Wearables: A Systematic Review with Meta-analysis and Expert Statement of the INTERLIVE Network. Sports Med 52, 1577–1597 (2022). https://doi.org/10.1007/s40279-021-01639-y.
- “21 CFR Part 868 — Anesthesiology Devices; §868.1730 Oxygen Uptake Computer.” Journal/Organization: U.S. Electronic Code of Federal Regulations / FDA-regulated device classification https://www.ecfr.gov/current/title-21/chapter-I/subchapter-H/part-868.
- Mehra M, Canter C, Hannan M, et al. The 2016 International Society for Heart Lung Transplantation listing criteria for heart transplantation: A 10-year update. The Journal of Heart and Lung Transplantation, 35, 1-23 https://doi.org/10.1016/j.healun.2015.10.023.
- Austin C. Hogwood, Krzysztof Smarż, Michele Golino, et al. Determinants of cardiorespiratory fitness after successfully reperfused ST-elevation myocardial infarction, Current Problems in Cardiology, 51, 10, (103382), (2026).https://doi.org/10.1016/j.cpcardiol.2026.103382