
Intoduction
For most of human history, sleep was treated as biological downtime, a dark, largely inaccessible interval between two productive days.
That view is rapidly becoming obsolete.
Sleep is emerging as one of medicine’s richest sources of physiological information. During the night, the brain cycles through distinct electrical states: breathing, heart rate and autonomic tone fluctuate, memories are reorganised, metabolic signals change, and the immune and endocrine systems undergo tightly timed recalibration.
Until recently, studying these processes required a patient to spend a night in a sleep laboratory, connected to multiple sensors. The test was detailed but inconvenient, expensive, and limited to a single artificial night.
The future of sleep will be different. It will be continuous, personalised, predictive, and eventually modifiable in real time.
The bed may become a diagnostic platform. A smartwatch may identify abnormal breathing before symptoms become obvious. Artificial intelligence may detect disease patterns hidden within a night of physiological data. Digital therapeutics may deliver behavioural treatment at scale. New drugs will target the biology of wakefulness rather than simply sedating the brain. And closed-loop systems may one day recognise a specific sleep state and intervene at precisely the right moment.
The central transformation is simple: We are moving from measuring how long someone sleeps to understanding what their sleeping body is telling us.










- Sleep is emerging as one of medicine’s richest sources of physiological information.
- The future of sleep will be different. It will be continuous, personalised, predictive, and eventually modifiable in real time.
- We are moving from measuring how long someone sleeps to understanding what their sleeping body is telling us.
Sleep is Becoming a Health Vital Sign
Medicine routinely measures blood pressure, pulse, temperature and oxygen saturation. Sleep has rarely been treated with the same seriousness, partly because it has been difficult to measure outside specialist centres.
Long-term wearable data are beginning to change that.
Research linking commercial wearable recordings with electronic health records suggests that sleep duration alone is not the whole story. Sleep regularity, timing and physiological structure may also be associated with the future development of chronic disease.
This has important implications. A person who sleeps seven hours at inconsistent times may not have the same biological profile as someone who sleeps seven regular hours. Two people with identical sleep duration may differ substantially in sleep fragmentation, respiratory disturbance, autonomic recovery and circadian alignment.
The future sleep assessment will therefore move beyond a single number.
It may include:
- Sleep duration and regularity
- Sleep and wake timing
- Night-time heart rate and heart-rate variability
- Respiratory patterns and oxygen fluctuations
- Movement and awakenings
- Temperature rhythms
- Circadian timing
- Daytime alertness and cognitive performance
Sleep could become a longitudinal biomarker of how the brain, cardiovascular system and metabolism are coping with life.
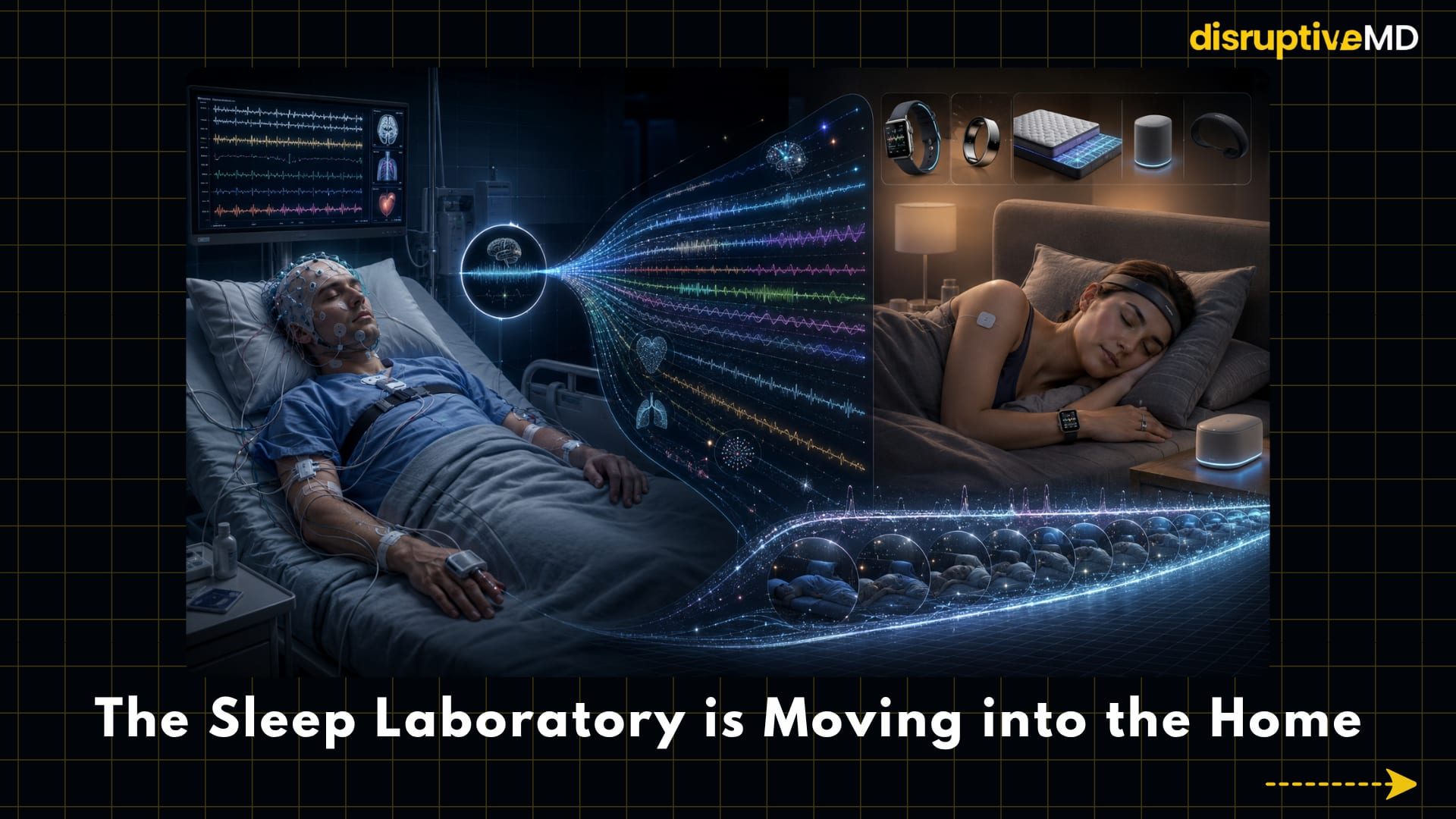
The Sleep Laboratory is Moving Into The Home
Polysomnography remains the clinical reference standard for detailed sleep assessment. It records brain activity, eye movements, muscle tone, breathing, heart rhythm and oxygenation.
But it captures only one or two nights.
Consumer wearables and home sensors can collect hundreds of nights of data. Watches and rings combine movement with optical pulse signals. Smart mattresses and bedside devices may track breathing without being attached to the body. Emerging patches and headbands can incorporate simplified electroencephalography, temperature or biochemical sensing.
This shift from a snapshot to a continuous movie may be transformative.
A single laboratory night can identify obstructive sleep apnoea or unusual neurological events. Months of home data may reveal something different: progressive sleep disruption, changing circadian behaviour, treatment response or deterioration associated with illness.
However, the distinction between wellness tracking and medical diagnosis remains crucial.
Consumer devices generally perform better at estimating whether a person is asleep than at accurately distinguishing individual sleep stages. Accuracy varies across devices, algorithms, populations and clinical conditions. A beautifully presented sleep score is not the same as a validated medical measurement.
The future is therefore unlikely to be one device replacing the sleep laboratory. It will be a layered system: continuous home monitoring for screening and trends, and followed by targeted clinical testing when necessary.
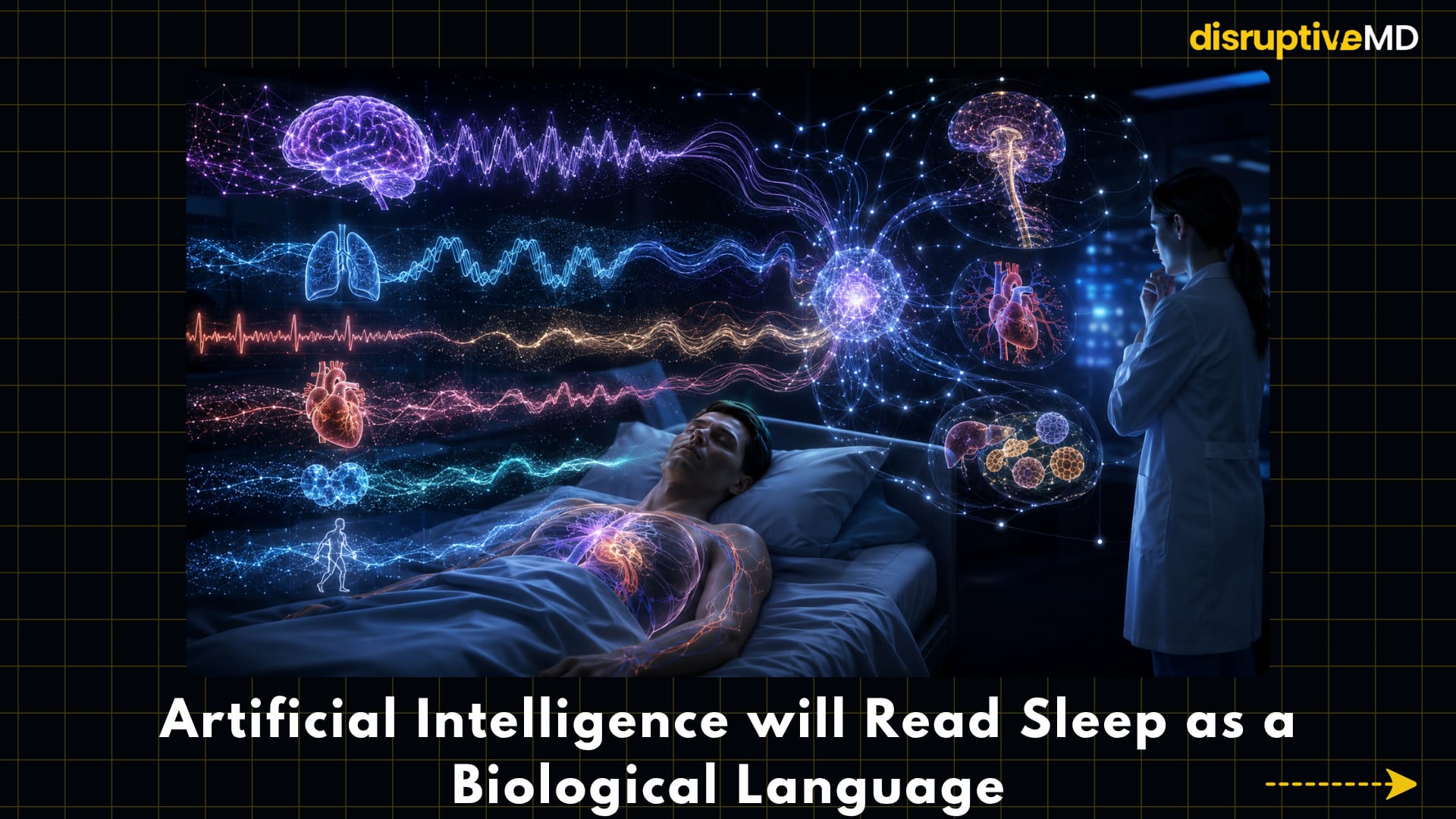
Artificial intelligence will read sleep as a biological language
A modern sleep study contains enormous amounts of information, far more than can be represented by manually labelling sleep as light, deep or rapid eye movement sleep.
Artificial intelligence can analyse relationships between brain waves, respiratory events, heart-rate changes, oxygen fluctuations, movement and arousals across an entire night. It can automate sleep staging and event detection, but its greater potential lies in discovering patterns humans do not routinely recognise.
A striking example is the development of large “foundation models” trained on multimodal sleep recordings. In early research, one such model used a single night of clinical sleep data to predict the future risk of numerous medical conditions, including cardiovascular, neurological and metabolic disorders [3].
This does not mean one night of sleep can definitively diagnose a person’s future. These are predictive associations that require external validation, careful calibration and prospective clinical testing.
But the direction is important.
The sleep study of the future may not merely say: “You have sleep apnoea.” It may also estimate: “This pattern is associated with elevated neurological or cardiovascular risk, and these are the features driving that estimate.”
For this to become responsible medicine, AI models will need to be explainable, validated across diverse populations and integrated into clinical decisions without creating false alarms.
Sleep treatment is moving from sedation to precision neurobiology
Traditional sleeping medications often work by broadly suppressing central nervous system activity. They may help initiate sleep, but sedation is not necessarily equivalent to restoring normal sleep physiology.
One of the most significant advances has been the targeting of the orexin system.
Orexin is a neurochemical involved in maintaining wakefulness. Dual orexin receptor antagonists treat insomnia by reducing wake-promoting signalling rather than simply enhancing generalised sedation. This represents a more biologically directed approach to insomnia.
The opposite strategy may help people with narcolepsy type 1, a condition characterised by profound orexin deficiency. Investigational orexin receptor agonists aim to restore wakefulness by addressing a central disease mechanism. Phase 2 studies of oveporexton reported improvements in wakefulness, sleepiness and cataplexy; subsequent phase 3 findings have also been reported, although regulatory review and longer-term evidence remain important.
These developments illustrate a wider transition: Future sleep medicines will increasingly target specific neural circuits, receptors and circadian mechanisms rather than treating all sleep problems as the same disorder.
Insomnia Care Will Become Digital, But Human Judgement Will Remain Essential
Cognitive behavioural therapy for insomnia, or CBT-I, is an evidence-based treatment for chronic insomnia. It addresses maladaptive sleep behaviours, irregular schedules, conditioned arousal and unhelpful beliefs about sleep.
Its major limitation is access. There are not enough trained clinicians to deliver it to every person who needs it.
Digital CBT-I can deliver structured behavioural therapy through apps or online platforms. Reviews indicate that digital treatment can improve insomnia and may offer an effective, scalable alternative when face-to-face therapy is unavailable, although personal support and clinical oversight may improve engagement for some patients.
The next generation will go beyond static lessons.
A future system could combine wearable data, light exposure, activity, mood and self-reported symptoms to adapt recommendations dynamically. Instead of providing generic sleep hygiene advice, it might detect that a person’s main problem is circadian delay, excessive time in bed, irregular wake time, evening light exposure or anxiety associated with attempted sleep.
Importantly, digital treatment should not become an excuse to overlook depression, medication effects, restless legs syndrome, sleep apnoea or other medical causes of disturbed sleep.
Technology should improve access and not remove clinical reasoning.
Obstructive Sleep Apnoea is Becoming a Metabolic Disease as Well as an Airway Disease
Obstructive sleep apnoea has traditionally been managed by preventing upper-airway collapse, most commonly with positive airway pressure devices. Other approaches include oral appliances, positional therapy, surgery and hypoglossal nerve stimulation in selected patients.
A major shift occurred when tirzepatide became the first medication approved by the US Food and Drug Administration specifically for moderate-to-severe obstructive sleep apnoea in adults with obesity, alongside reduced-calorie nutrition and physical activity.
This matters because it recognises that sleep apnoea is not only an anatomical airway problem. In many patients, it is also influenced by obesity, fat distribution, metabolic health and systemic inflammation.
Future management may combine:
- Airway support
- Metabolic therapy
- Weight reduction
- Anatomical phenotyping
- Positional and behavioural interventions
- Neuromodulation
- Personalised surgical planning
Rather than prescribing the same device to every patient, clinicians may increasingly classify sleep apnoea according to its underlying mechanism.
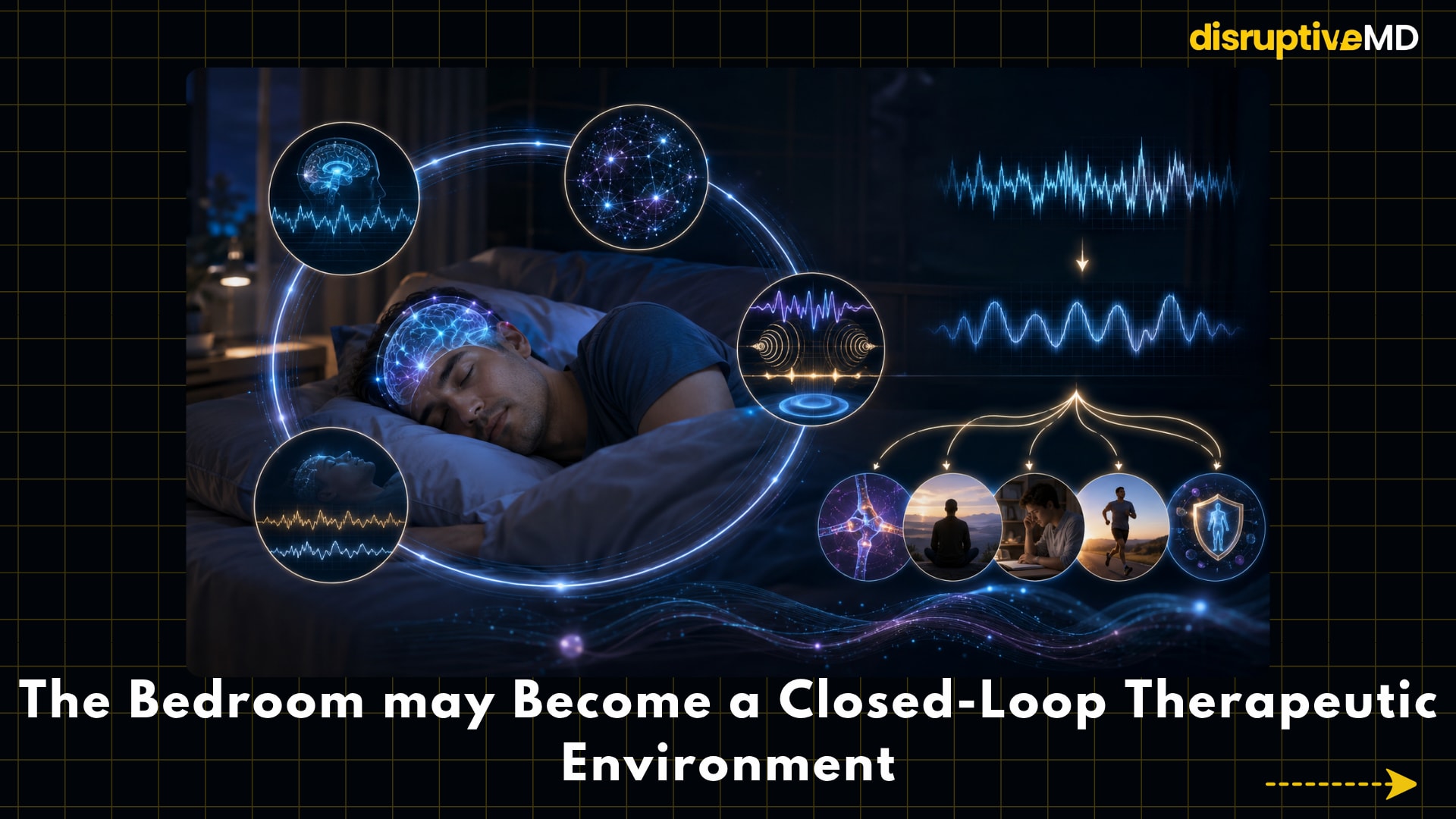
The Bedroom May Become a Closed-Loop Therapeutic Environment
Most current sleep technologies are open loop: they deliver the same sound, temperature, light or stimulation regardless of what the brain is doing.
Closed-loop systems work differently.
They continuously detect physiological state and intervene only when the timing is appropriate. For example, a system could identify slow-wave sleep and deliver precisely timed soft sounds intended to enhance slow oscillations. Other experimental approaches use electrical, sensory or acoustic stimulation synchronised to brain activity.
Research into closed-loop auditory stimulation suggests that it can alter slow-wave activity, but results for memory and clinical outcomes remain inconsistent. Non-invasive brain stimulation is scientifically promising, yet it has not reached the point of established routine treatment for sleep disorders.
This is an area where marketing is moving faster than medicine.
The concept is powerful: sense the sleeping brain, interpret its state, and intervene and verify the response. But meaningful endpoints like better memory, improved daytime function, and reduced disease risk matter more than simply changing a waveform.
Circadian Medicine May Become as Important as Sleep Medicine
Sleep is governed by two interacting systems: the pressure to sleep that builds during wakefulness, and the circadian clock that determines when the body expects sleep and wakefulness.
Modern life frequently separates the two.
Artificial light, shift work, late-night screens, travel and irregular schedules can produce circadian misalignment. A person may be tired yet biologically mistimed for sleep.
Future treatment will increasingly consider when an intervention is delivered, not merely what it is.
Light exposure, exercise, meals, melatonin and medication all have timing-dependent effects. Wearable light sensors and temperature or activity rhythms may help estimate individual circadian phase. Early digital systems are already testing personalised coaching based on wearable and environmental light data.
The future prescription may therefore look less like: “Sleep for eight hours.” And more like: “Wake at this time, obtain bright light during this window, exercise before this point, reduce light after this hour and shift your schedule gradually over six days.”
Chronotherapy could become particularly relevant for athletes, shift workers, adolescents, frequent travellers and people with mood disorders.
Athletes Will Train Sleep as Deliberately as Strength
Elite sport increasingly recognises sleep as part of the training programme rather than passive recovery after it.
For athletes, sleep affects reaction time, learning, immune function, pain perception, glycogen restoration, decision-making and subjective recovery. Travel, late competition schedules, pre-event anxiety and early training can all disrupt it.
Future athlete management may integrate sleep regularity, nocturnal physiology, training load, travel schedules and performance testing. AI systems may identify an athlete whose recovery is deteriorating before performance visibly declines.
But there is a danger: data can create anxiety.
An athlete who feels recovered may become distressed after receiving a low sleep score from a consumer device. This phenomenon, sometimes called orthosomnia, illustrates how excessive pursuit of perfect sleep can itself interfere with sleep.
The goal should not be perfect numbers. It should be better recovery, health and performance.
The Next Great Sleep Device May be The Room Itself
Future bedrooms may automatically adjust light, sound, temperature and airflow according to circadian timing and sleep state.
Smart environments could:
- Reduce blue-enriched light before bedtime
- Lower room temperature during sleep initiation
- Detect snoring or abnormal breathing
- Alter bed position during airway obstruction
- Introduce morning light at an appropriate circadian phase
- Share clinically relevant trends with healthcare teams
Such systems could be especially valuable for older adults and people with chronic disease.
Yet they also raise an uncomfortable question: Who owns the data generated while we sleep?
Sleep data may reveal pregnancy, alcohol use, respiratory disease, mental-health patterns, medication effects or early neurological change. Insurers, employers, technology companies and sporting organisations could all find such information valuable.
Privacy cannot be treated as an afterthought. The future of sleep technology must include informed consent, secure storage, transparent algorithms and clear limits on secondary data use.
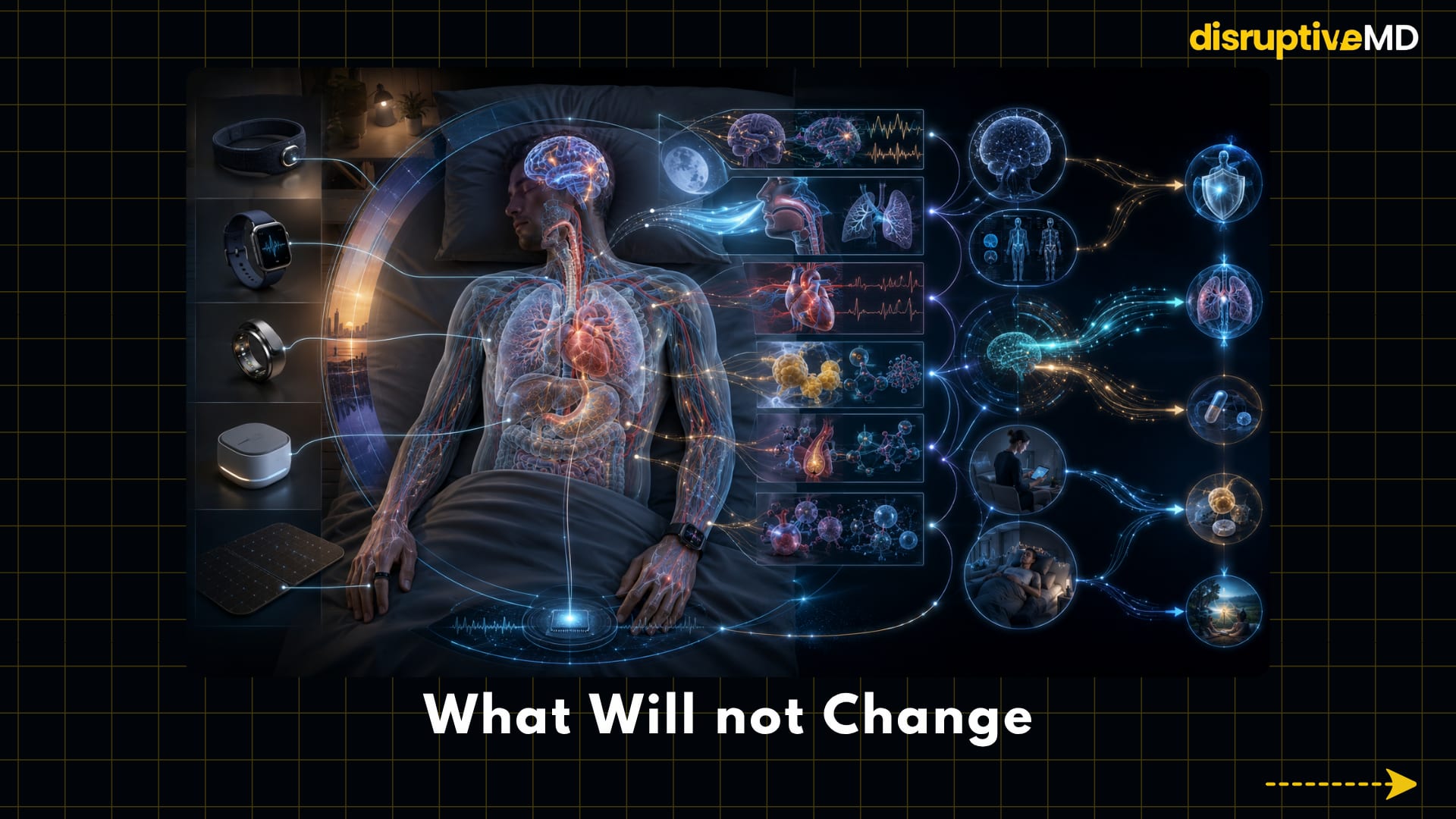
What Will Not Change
Despite rapid innovation, the fundamentals of healthy sleep remain remarkably resistant to disruption.
No algorithm can fully compensate for chronic sleep deprivation. No supplement can reliably neutralise an irregular schedule. No expensive mattress can correct untreated sleep apnoea. No sleep score is more important than persistent daytime sleepiness, witnessed breathing pauses or a dangerous loss of alertness while driving.
The foundations remain:
- Adequate sleep opportunity
- A reasonably regular wake time
- Appropriate light exposure
- Physical activity
- Management of medical and psychological disorders
- Limiting substances and behaviours that disrupt sleep
- Evidence-based treatment when a sleep disorder is present
Technology will become most useful when it strengthens these fundamentals rather than distracting from them.
The Future Is Not Merely Better Sleep Tracking
The most important change will not be that devices become better at telling us when we fell asleep.
It will be that sleep becomes a platform for prevention, diagnosis and personalised treatment.
The future may allow us to detect disease through the sleeping body, treat insomnia at scale, classify sleep apnoea by mechanism, repair specific neurochemical deficits, align therapy with circadian timing and interact with sleeping brain activity in real time.
But cutting-edge sleep medicine must remain evidence-led.
A device that measures more is not automatically a device that improves health. A change in deep-sleep percentage is not automatically a meaningful clinical benefit. And artificial intelligence that predicts risk is not useful unless it leads to an intervention that improves outcomes.
The real future of sleep is therefore not simply technological. It is the transformation of sleep from an ignored biological interval into an active component of precision medicine.
Tomorrow’s medicine may discover that one of the clearest windows into waking health opens only after we close our eyes.
Evidence Base
Long-term wearable research supports evaluating not only sleep duration but also sleep stages and regularity, although these associations do not by themselves prove causation.
Wearable sleep-stage estimates remain inconsistent across devices and sensor combinations. Reviews show growing potential for home monitoring but emphasise accuracy, validation and generalisability limitations.
The SleepFM study reported that a multimodal AI model could predict a broad range of future conditions from clinical sleep recordings. This is a research prediction model, not a standalone diagnostic test.
Digital CBT-I is supported as a scalable treatment option, while established clinical guidance continues to recommend behavioural and psychological therapy for chronic insomnia.
Orexin receptor antagonists represent a mechanism-based treatment for insomnia. Oveporexton, an investigational orexin agonist, improved narcolepsy type 1 outcomes in a published phase 2 trial; later phase 3 findings have been reported but should be interpreted pending full peer-reviewed publication and regulatory review.
On December 20, 2024, the FDA approved tirzepatide for moderate-to-severe obstructive sleep apnoea in adults with obesity, alongside diet and physical activity.
Closed-loop auditory and non-invasive brain stimulation remain promising but experimental. Reviews report mixed outcome data and conclude that brain stimulation has not yet produced established evidence-based sleep treatments.
References
- Zheng NS, Annis J, Master H, et al. Sleep patterns and risk of chronic disease as measured by long-term monitoring with commercial wearable devices in the All of Us Research Program. Nature Medicine. 2024;30:2648–2656. DOI: https://doi.org/10.1038/s41591-024-03155-8.
- Birrer V, Elgendi M, Lambercy O, Menon C. Evaluating reliability in wearable devices for sleep staging. npj Digital Medicine. 2024;7:74. DOI: https://doi.org/10.1038/s41746-024-01016-9.
- Thapa R, Kjaer MR, He B, et al. A multimodal sleep foundation model for disease prediction. Nature Medicine.2026;32:752–762. DOI: https://doi.org/10.1038/s41591-025-04133-4.
- Kishi T, Koebis M, Sugawara M, et al. Orexin receptor antagonists in the treatment of insomnia associated with psychiatric disorders: a systematic review. Translational Psychiatry. 2024;14:374. DOI: https://doi.org/10.1038/s41398-024-03087-4.
- Dauvilliers Y, Plazzi G, Mignot E, et al. Oveporexton, an oral orexin receptor 2–selective agonist, in narcolepsy type 1. New England Journal of Medicine. 2025;392(19):1905–1916. DOI: https://doi.org/10.1056/NEJMoa2405847.
- Li C, Luo Q, Wu H. Digital therapeutics for insomnia: an umbrella review and meta-meta-analysis. npj Digital Medicine.2025;8:554. DOI: https://doi.org/10.1038/s41746-025-01946-y.
- U.S. Food and Drug Administration. FDA Approves First Medication for Obstructive Sleep Apnea. Published December 20, 2024. Official FDA link: https://www.fda.gov/news-events/press-announcements/fda-approves-first-medication-obstructive-sleep-apnea.
- Coon WG, Nilsson SJ, Smith MT, Reid MJ. Acoustic stimulation and other emerging approaches to enhance sleep: design notes for the next generation of closed-loop neurostimulation technology. Frontiers in Neuroscience.2026;19:1682450. DOI: https://doi.org/10.3389/fnins.2025.1682450.
- Krone LB, Song SH, Jaramillo V, Violante IR. The future of non-invasive brain stimulation in sleep medicine. Journal of Sleep Research. 2025;34(5):e70071. DOI: https://doi.org/10.1111/jsr.70071.
- Seo M, Park S, Jeong J, et al. The Circadian Rhythm for Sleep digital therapeutic for insomnia: conceptual background and single-arm feasibility study. DIGITAL HEALTH. 2026;12:20552076261430230. DOI: https://doi.org/10.1177/20552076261430230.