
Introduction
Eye surgery is entering a new era where the goal is not just to regain sight but to make delicate operations more precise, less intrusive, more personal and more scalable. This is important since the loss of vision is one of the leading worldwide health problems. The World Health Organization estimates that at least 2.2 billion individuals have near or distance visual impairment and at least 1 billion of these cases might have been prevented or still need to be addressed. Refractive error and cataract are the main causes of visual impairment and blindness worldwide. Glaucoma, diabetic retinopathy and age-related macular degeneration remain major sources of irreversible visual handicap if diagnosis or treatment is delayed.
The most important developments in ocular surgery are not just new devices. They indicate a move away from “manual removal or repair” and towards image-guided, microincisional, biologically targeted, and digitally assisted surgery. The eye is a particularly demanding organ, as features including the cornea, lens capsule, retina, optic nerve and macula are measured in microns and very slight inaccuracies can impair vision. The five breakthroughs below are disruptive in that they affect what surgeons can see, where they can operate, how early disease can be treated, and how recovery and risk could be managed.
Why Ophthalmic Surgery Needed a Precision Upgrade
Precision has traditionally been the hallmark of ophthalmic surgery. Vision depends on clear tissues, precise focusing, healthy retinal nerve tissue and stable intraocular pressure. Cataract is a clouding of the natural lens of the eye. Refractive error means that light is not focused properly on the retina. Glaucoma is a progressive optic neuropathy (damage to the optic nerve) often associated with increased intraocular pressure. Inherited retinal dystrophy is a genetic disease where the light sensing cells of the retina progressively fail. These disorders are frequent and can have a variety of clinical pictures. They are often managed surgically when drugs, spectacles or observation are not enough.
The key question in modern eye surgery is no longer only whether an operation is possible. It is whether we can make surgery safer, more reproducible, less dependent on massive incisions, better directed by real-time imaging and able to deliver advanced medicines such as genes or cells to the exact retinal layer where disease starts. This matters because ophthalmic treatment must meet two very distinct demands simultaneously: high-volume public-health operations such as cataract surgery and highly specialized microsurgery for rare or severe retinal disease.
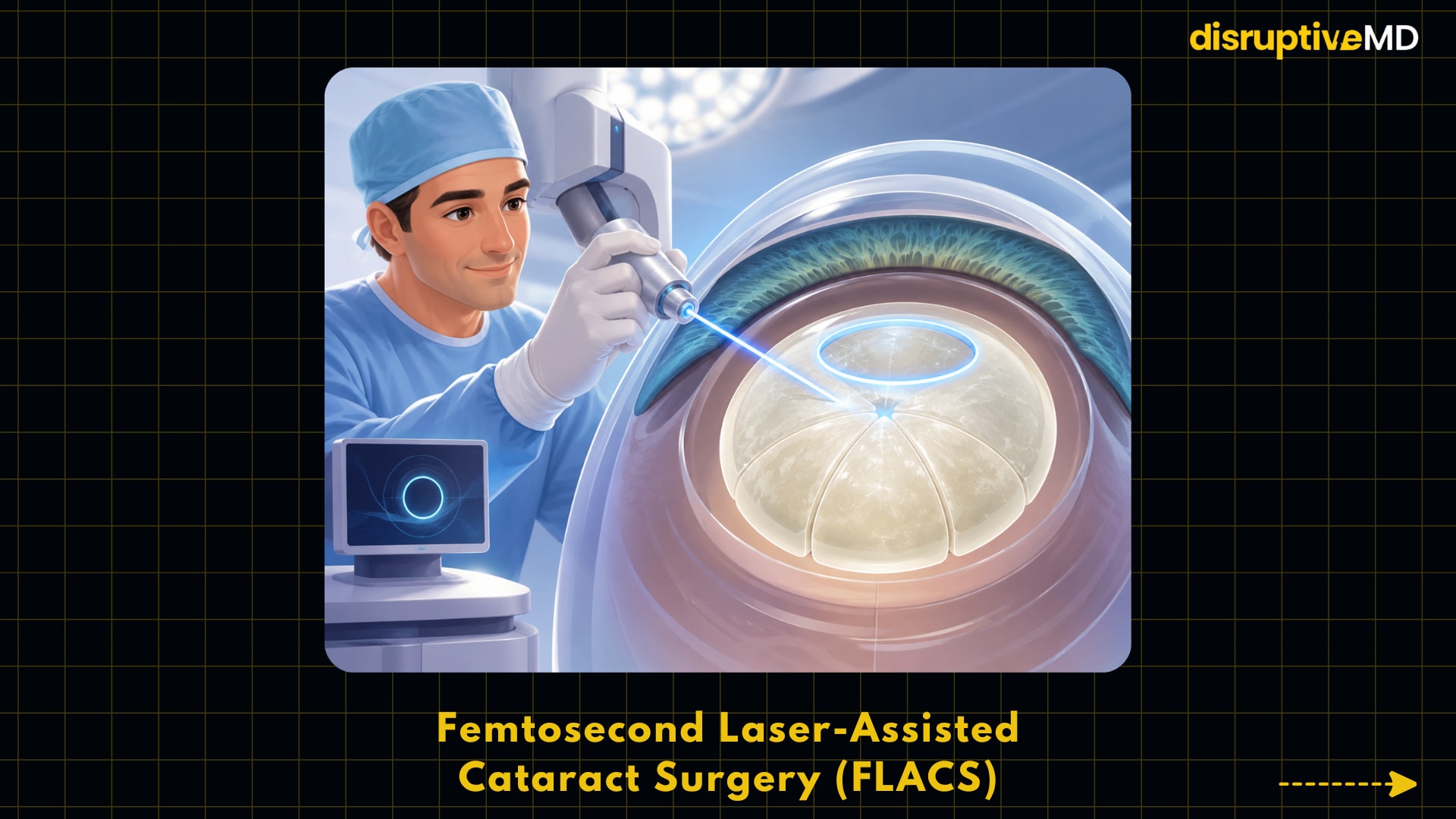
- Femtosecond laser-assisted cataract surgery uses ultrafast laser pulses for corneal incisions, capsulotomy, and lens fragmentation.
- The technology can standardize technically difficult steps, especially in complex eyes.
- Current evidence shows FLACS is not generally superior to high-quality conventional phacoemulsification in routine cataract surgery.
What the Top 5 Innovations Do
1. Femtosecond Laser-Assisted Cataract Surgery (FLACS): Automating the Most Delicate Steps
Femtosecond laser-assisted cataract surgery (FLACS) employs ultrafast laser pulses to accomplish some aspects of cataract surgery, such as corneal incisions, capsulotomy and lens fragmentation. The capsulotomy is the circular incision produced in the thin capsule that surrounds the hazy lens. Fragmentation of the lens is the division of the cataract before its removal by ultrasound-based phacoemulsification. FLACS is attractive because it can standardize stages that are technically difficult, especially in complex eyes. However, substantial randomized data have shown that it has not replaced conventional phacoemulsification in regular cataract surgery. In the UK FACT randomised non-inferiority trial, 785 individuals were randomised to FLACS or conventional phacoemulsification with identical visual outcomes at 3 and 12 months however the study also showed that FLACS was not cost-effective in that environment. The significance of this discovery lies in the fact that cataract surgery is one of the most common surgeries performed worldwide and even tiny workflow improvements potentially affect millions of patients. The main lesson is balanced: FLACS is technically clever and may aid in specific cases, but existing evidence does not justify calling it better than high quality manual phacoemulsification.
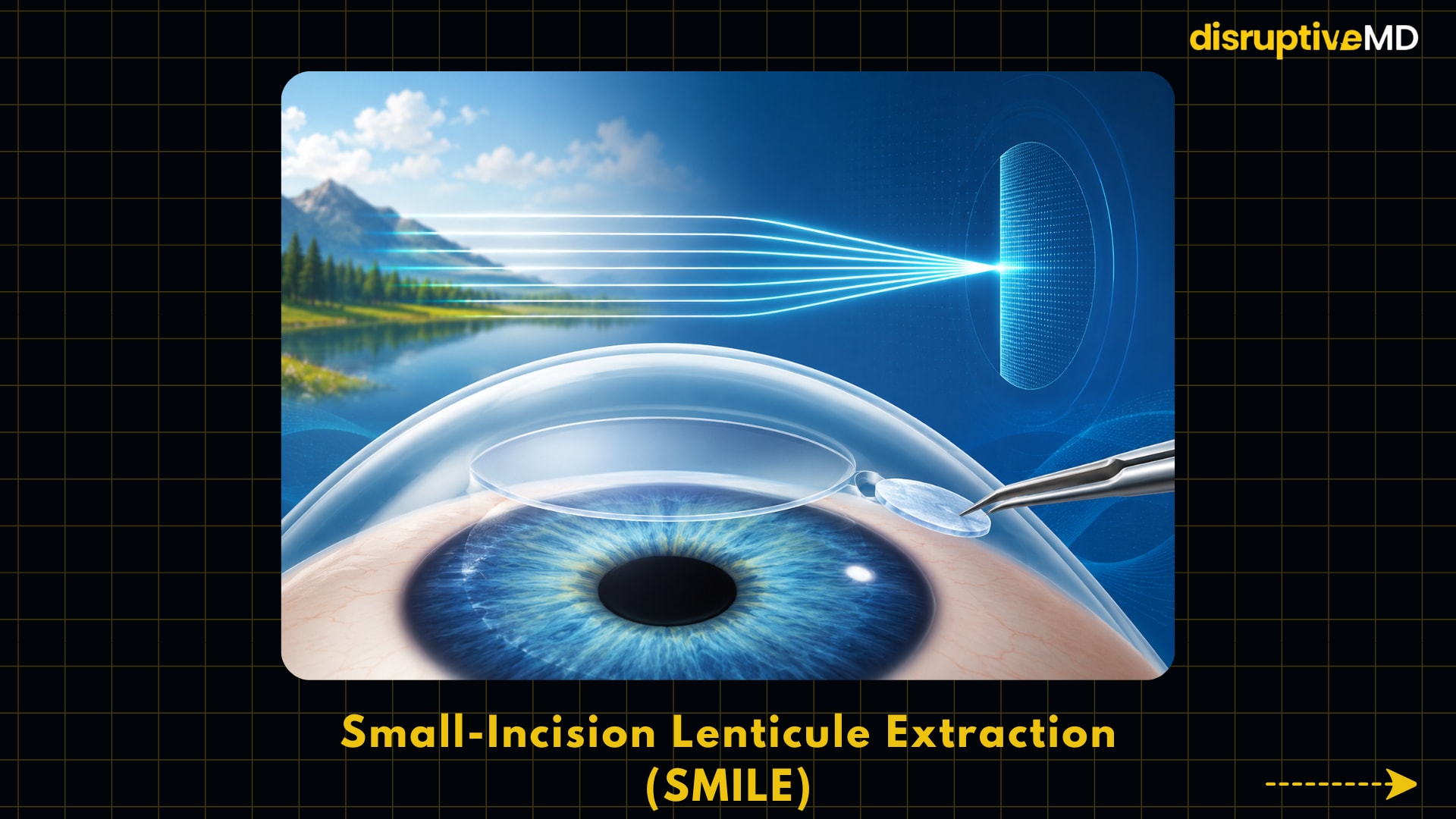
2. Small-Incision Lenticule Extraction (SMILE): Refractive Surgery Without a Corneal Flap
Small incision lenticule extraction, or SMILE, is a corneal refractive surgery that corrects myopia, or short-sightedness, by creating a thin disc of tissue inside the cornea called a lenticule with a femtosecond laser. The surgeon then removes that lenticule by a small incision and reshapes the cornea so that light is focused more properly on the retina. Unlike LASIK, SMILE does not involve the formation of a bigger corneal flap, which is why researchers have explored whether it may lessen some flap-related risks and ocular surface symptoms. In 2024, a meta-analysis of randomized controlled trials showed that SMILE had broadly comparable efficacy, safety, predictability, and stability compared with other corneal refractive procedures for myopia, with less influence on corneal sensation and corneal nerve density in the included studies.
And this is important because refractive surgery stands at the intersection of medicine, technology and quality of life. Corneal thickness, corneal shape, dry eye status and patient expectations are still important factors for determining suitability, so SMILE does not mean that thorough screening is no longer necessary. However, it has changed the surgical design of laser vision correction as more of the procedure is now done inside the corneal tissue rather than under a flap.
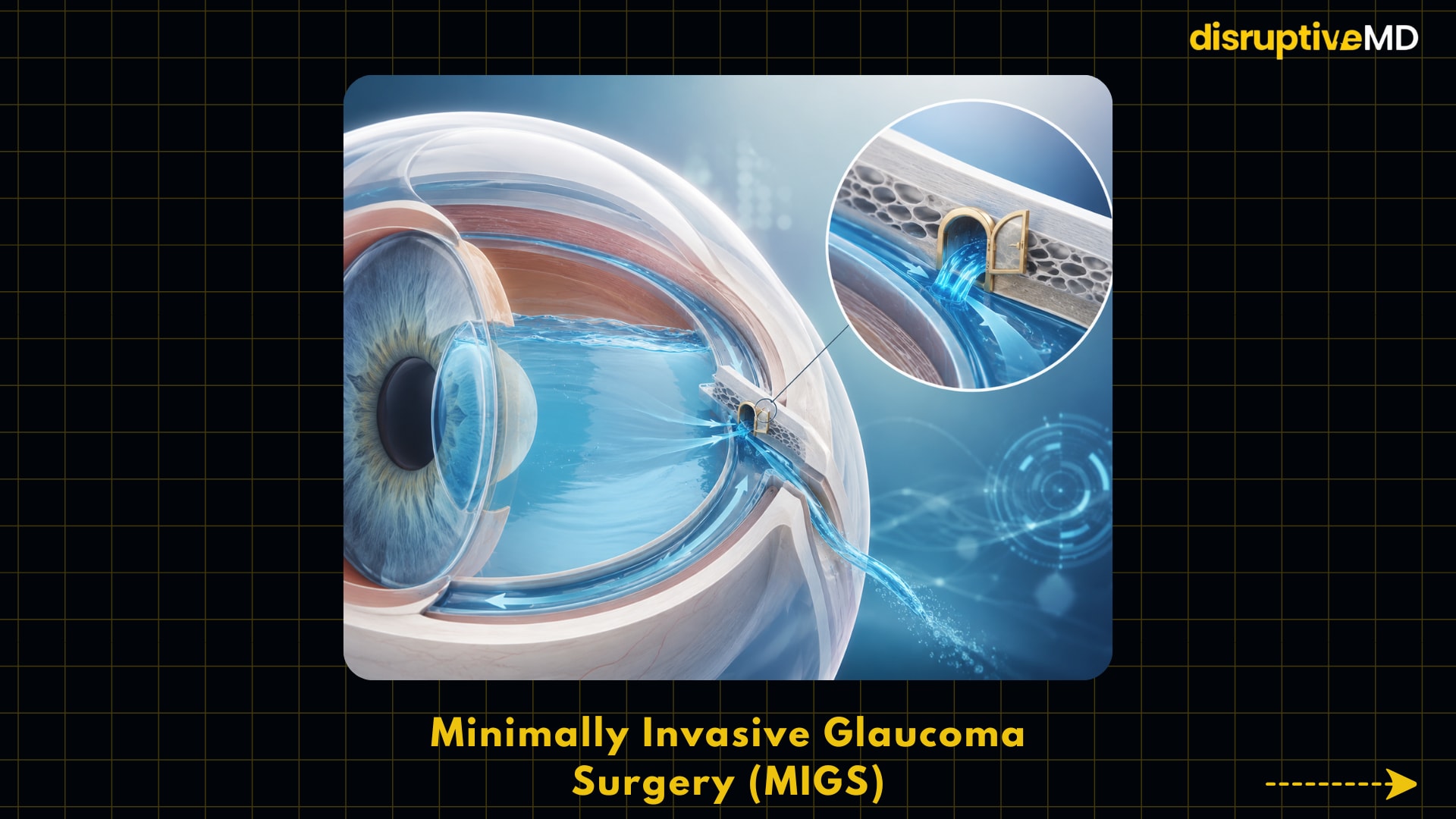
3. Minimally Invasive Glaucoma Surgery (MIGS): Lowering Eye Pressure with Smaller Anatomical Disruption
Minimally invasive glaucoma surgery, or MIGS, is a series of microincisional techniques meant to lower intraocular pressure by increasing drainage of the aqueous humour, the clear fluid that fills the eye. Many of the MIGS techniques, such as the Trabectome, focus on the trabecular meshwork and Schlemm canal, which is part of the natural drainage channel of the eye, as opposed to building a big external filtering route as in standard trabeculectomy. Why does this matter? Many patients struggle with daily drops, side effects, expense or adherence, although glaucoma management is often a long-term pressure reduction. A summary of six Cochrane systematic reviews published in JAMA Ophthalmology found that the addition of some trabecular bypass devices to cataract surgery improved medication-free glaucoma control compared to cataract surgery alone, but the pressure-lowering effect was modest and the quality of evidence was better for some devices than others. MIGS is disruptive in that it has moved glaucoma surgery earlier in the disease timeline for select patients, particularly those with mild to moderate open-angle glaucoma undergoing cataract surgery. The restriction is equally important: MIGS in general does not drop intraocular pressure as substantially as standard filtering surgery, hence may not be suited for advanced glaucoma requiring very low goal pressures.
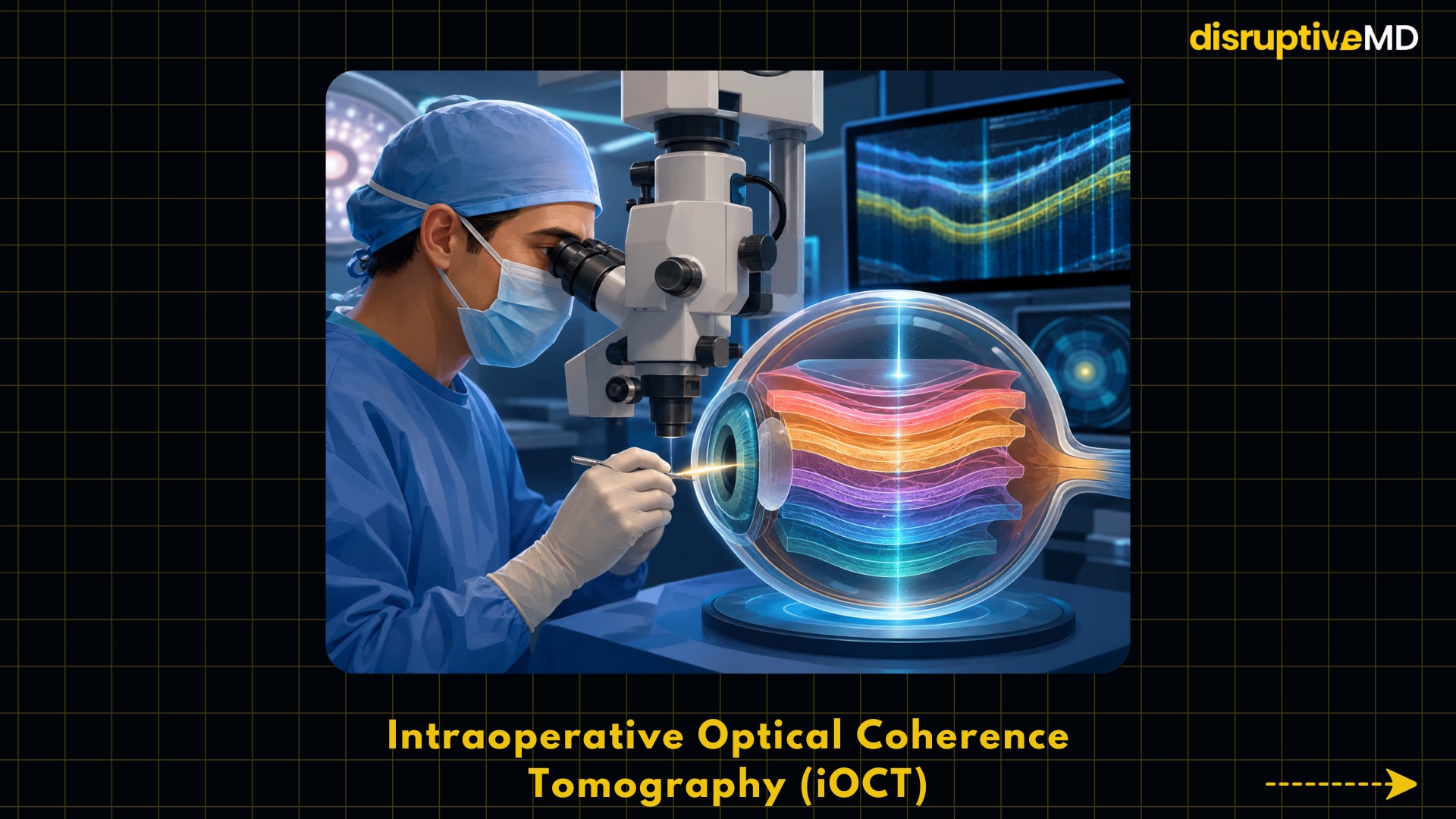
4. Intraoperative Optical Coherence Tomography (iOCT): Seeing Microscopic Tissue Layers During Surgery
Intraoperative optical coherence tomography (iOCT) is high-resolution cross-sectional imaging brought to the operating room. Optical coherence tomography is essentially an optical ultrasound, using light instead of sound to produce detailed images of retinal, corneal or other ocular layers. In retinal membrane peeling, corneal transplantation, or complex vitreoretinal surgery, iOCT can demonstrate if tissue has been completely detached, if fluid is in the wrong layer, or if the surgical plane is safe. In the PIONEER research, intraoperative OCT imaging was achieved in 518 of 531 participating eyes, or 98%, and surgeon comments suggested it informed decision-making in 48% of lamellar keratoplasty cases and 43% of membrane peeling procedures. This is important because ophthalmic surgeons generally employ surface views from the microscope, yet many surgical choices are made in three-dimensional layers of tissue that cannot be fully seen from the surface. While iOCT does not always improve outcomes in all cases, it turns surgery from a purely visual-manual technique to a real-time image-guided procedure, especially when tissue boundaries are fragile or ambiguous.
5. Subretinal Gene Therapy and Robotic Precision Surgery: Turning Surgery Into a Treatment-Delivery Platform
Subretinal gene therapy is a surgical procedure to inject a therapeutic genetic vector underneath the retina, in close proximity to the retinal pigment epithelium and photoreceptors, sites of origin of many inherited retinal illnesses. The best recognized example is voretigene neparvovec-rzyl, an adeno-associated virus vector gene therapy approved by the US Food and Drug Administration for individuals with verified biallelic RPE65 mutation-associated retinal degeneration. “Bi-allelic” indicates both copies of the RPE65 gene are impacted and the therapy is designed for patients who have viable retinal cells remaining. The evidence base is minimal yet of clinical importance as rare hereditary retinal disorders have limited patient populations. The main phase 3 clinical trial of voretigene neparvovec was an open-label randomized controlled trial in patients with RPE65-mediated inherited retinal dystrophy, and supporting evidence includes functional vision testing using the multi-luminance mobility test, which measures the ability to navigate under different lighting conditions. It matters because surgery is not just about cutting out diseased tissue or fixing anatomy anymore but, in selected retinal illnesses, it can deliver a molecular therapeutic straight into the damaged tissue compartment. Robotic-assisted vitreoretinal surgery is still in its infancy, but it is heading in the same direction: stabilizing hand movements and scaling them for treatments that require more accuracy than is normally possible for humans to achieve manually. A first-in-human study described remotely-controlled robot-assisted retinal surgery with a telemanipulation device and subsequent randomized work compared robot-assisted to manual epiretinal membrane peeling. The real-world importance is not that robots are replacing ophthalmic surgeons, but that robotic systems may ultimately enable ultra-precise operations such as subretinal injections, retinal vein cannulation or cell therapy delivery.
Evidence and Real-World Meaning
These innovations are not uniformly distributed, with the strongest real-world evidence among them. FLACS and SMILE have randomized and meta-analytic evidence, but with different implications. FLACS improves automation of cataract steps, but without a clear advantage over conventional phacoemulsification in routine cases. SMILE is a validated alternative design for myopic laser refractive surgery with comparable outcomes to established procedures. MIGS has revolutionized the treatment of glaucoma, offering a less invasive surgical alternative for appropriate individuals, especially when performed with cataract surgery. However, the most rigorous data synthesis suggests little pressure reduction and device-specific evidence varies thus the clinical decision is not “MIGS or no MIGS” but what patient, illness stage, pressure aim and medication load justifies the surgery. There is significant evidence for the feasibility and intraoperative usefulness of iOCT, particularly for procedures where the layers of the tissue are difficult to judge with the microscope alone. This is a crucial distinction for health systems considering investing in pricey imaging platforms, as the existing data favours improved surgical information and decision-making above universal improvement in long-term visual outcomes. The most obvious example of ocular surgery as a biologic delivery platform is subretinal gene therapy. FDA authorized RPE65 gene therapy is proof that retinal surgery can offer a treatment based on a genetic mechanism and not just an anatomical problem, however the eligible group is small and long-term durability, access and cost remain key issues.
Limitations, Risks, and Unanswered Questions
Many surgical breakthroughs are hampered by the fact that technical beauty does not always translate to superior patient outcomes. FLACS is a perfect example of this: it can automate challenging cataract steps, yet the FACT study showed equal visual outcomes and inferior cost-effectiveness compared to conventional phacoemulsification in the examined context. That matters, since health systems need to determine if the more cost platforms deliver enough therapeutic value to support more widespread deployment. MIGS asks a different question: How much pressure reduction is enough? Intraocular pressure is the primary modifiable risk factor in glaucoma, however advanced glaucoma may require lower goal pressures than may be reliably attained by current MIGS techniques. Reviews also highlight that the area of MIGS currently needs more long-term comparative randomized trials between device kinds, patient groups and illness stages. Patient selection is critical to SMILE and other refractive surgeries. A technically successful procedure may not be suitable for a patient with unstable refraction, thin or uneven corneas, considerable dry eye, early keratoconus or unrealistic expectations. The main restriction is that refractive surgery corrects optical focusing, but not the increasing myopia or ocular surface disease biology that underlies it. Clinical proof is not enough for the deployment of iOCT and robotic surgery. Challenges include equipment expense, integration into the operating room, training time, data interpretation, slower surgical processes in early adoption, and uncertain reimbursement. Compared to well-established ophthalmic operations, robot-assisted retinal treatments are still in the early stage; feasibility and safety of certain procedures have been confirmed in published research but superiority of outcomes has not been demonstrated broadly yet. Questions remain for gene therapy, too. Subretinal delivery involves specific surgical expertise, patients require genetic confirmation and viable retinal cells, and outcomes can vary depending on disease stage. And even when there is regulatory approval, access to rare-disease medicines can still be challenging due to the expense, specialist-centre requirements, follow-up requirements, and uncertainty about extremely long-term efficacy in varied populations.
Conclusion
The future of eye surgery will likely be more accurate, more image guided, more physiologically tailored and more customized. The most realistic hope is not that every new device will beat expert conventional surgery, but that selected innovations will improve care for selected patients: SMILE for appropriate refractive candidates, MIGS for selected glaucoma patients, iOCT for complex layer-based surgery, FLACS for specific cataract scenarios, and subretinal gene therapy for carefully diagnosed inherited retinal disease. The bigger picture is that eye surgery is shifting away from being a trade that relies heavily on hand skill to a hybrid discipline that integrates microsurgery, image science, genetics, robots, and health-system implementation. That transition is important for patients because vision is crucial to independence, for doctors because surgical choices are becoming data-rich, and for health systems because the worldwide burden of preventable or treatable vision impairment remains high.
Evidence Rating
Mixed or limited evidence. Some advances such as SMILE, selected MIGS devices, FLACS evidence comparisons and RPE65 gene therapy are supported by randomized clinical trials, meta-analyses and regulatory approval. Others, including intraoperative OCT and robotic-assisted vitreoretinal surgery, show significant evidence of feasibility and decision support but require broader evidence of long-term outcome benefit, cost-effectiveness, and scalability across different surgical contexts.
Educational Disclaimer
This material is for general informational purposes only and is not a substitute for professional medical advice, diagnosis or treatment. Patients should seek examination and care from qualified ophthalmologists or other appropriate health care providers.
References
- World Health Organization. Blindness and vision impairment. Updated February 10, 2026.
- Day AC, Burr JM, Bennett K, et al. Femtosecond laser-assisted cataract surgery compared with phacoemulsification: the FACT non-inferiority RCT. Southampton (UK): NIHR Journals Library; 2021 Jan. (Health Technology Assessment, No. 25.6.) Available from: https://www.ncbi.nlm.nih.gov/books/NBK567022/ doi: 10.3310/hta25060.
- Schweitzer C, Brezin A, Cochener B, Monnet D, Germain C, Roseng S, Sitta R, Maillard A, Hayes N, Denis P, Pisella PJ, Benard A; FEMCAT study group. Femtosecond laser-assisted versus phacoemulsification cataract surgery (FEMCAT): a multicentre participant-masked randomised superiority and cost-effectiveness trial. Lancet. 2020 Jan 18;395(10219):212-224. doi: 10.1016/S0140-6736(19)32481-X. PMID: 31954466.
- Liu, J., Lu, Y., Liu, J. et al. Meta-analysis of efficacy, safety, stability and predictability of Small Incision Lenticule Extraction (SMILE) for myopia. Lasers Med Sci 39, 57 (2024). https://doi.org/10.1007/s10103-024-04007-0.
- Moshirfar M, Somani SN, Patel BC. Small Incision Lenticule Extraction. [Updated 2024 Feb 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK549896/.
- Gillmann K, Mansouri K. Minimally Invasive Glaucoma Surgery: Where Is the Evidence? Asia Pac J Ophthalmol (Phila). 2020 May-Jun;9(3):203-214. doi: 10.1097/APO.0000000000000294. PMID: 32501895; PMCID: PMC7299223.
- Bicket AK, Le JT, Azuara-Blanco A, et al. Minimally Invasive Glaucoma Surgical Techniques for Open-Angle Glaucoma: An Overview of Cochrane Systematic Reviews and Network Meta-analysis. JAMA Ophthalmol. 2021;139(9):983–989. doi:10.1001/jamaophthalmol.2021.2351.
- Ehlers JP, Dupps WJ, Kaiser PK, Goshe J, Singh RP, Petkovsek D, Srivastava SK. The Prospective Intraoperative and Perioperative Ophthalmic ImagiNg with Optical CoherEncE TomogRaphy (PIONEER) Study: 2-year results. Am J Ophthalmol. 2014 Nov;158(5):999-1007. doi: 10.1016/j.ajo.2014.07.034. Epub 2014 Jul 29. PMID: 25077834; PMCID: PMC4250395.
- Ehlers JP, Modi YS, Pecen PE, Goshe J, Dupps WJ, Rachitskaya A, Sharma S, Yuan A, Singh R, Kaiser PK, Reese JL, Calabrise C, Watts A, Srivastava SK. The DISCOVER Study 3-Year Results: Feasibility and Usefulness of Microscope-Integrated Intraoperative OCT during Ophthalmic Surgery. Ophthalmology. 2018 Jul;125(7):1014-1027. doi: 10.1016/j.ophtha.2017.12.037. Epub 2018 Mar 2. PMID: 29409662; PMCID: PMC6015779.
- US Food and Drug Administration. LUXTURNA: voretigene neparvovec-rzyl product information and indication.
- Russell S, Bennett J, Wellman JA, Chung DC, Yu ZF, Tillman A, Wittes J, Pappas J, Elci O, McCague S, Cross D, Marshall KA, Walshire J, Kehoe TL, Reichert H, Davis M, Raffini L, George LA, Hudson FP, Dingfield L, Zhu X, Haller JA, Sohn EH, Mahajan VB, Pfeifer W, Weckmann M, Johnson C, Gewaily D, Drack A, Stone E, Wachtel K, Simonelli F, Leroy BP, Wright JF, High KA, Maguire AM. Efficacy and safety of voretigene neparvovec (AAV2-hRPE65v2) in patients with RPE65-mediated inherited retinal dystrophy: a randomised, controlled, open-label, phase 3 trial. Lancet. 2017 Aug 26;390(10097):849-860. doi: 10.1016/S0140-6736(17)31868-8. Epub 2017 Jul 14. Erratum in: Lancet. 2017 Aug 26;390(10097):848. doi: 10.1016/S0140-6736(17)32235-3. PMID: 28712537; PMCID: PMC5726391.
- Edwards TL, Xue K, Meenink HCM, Beelen MJ, Naus GJL, Simunovic MP, Latasiewicz M, Farmery AD, de Smet MD, MacLaren RE. First-in-human study of the safety and viability of intraocular robotic surgery. Nat Biomed Eng. 2018 Jun 18;2:649-656. doi: 10.1038/s41551-018-0248-4. PMID: 30263872; PMCID: PMC6155489.
- Faridpooya K, van Romunde SHM, Manning SS, van Meurs JC, Naus GJL, Beelen MJ, Meenink TCM, Smit J, de Smet MD. Randomised controlled trial on robot-assisted versus manual surgery for pucker peeling. Clin Exp Ophthalmol. 2022 Dec;50(9):1057-1064. doi: 10.1111/ceo.14174. Epub 2022 Oct 17. PMID: 36177965.