
Introduction
Laser eye surgery has moved from a simple promise of “removing glasses” to a more precise question: which corneal reshaping method gives the right balance of vision, safety, recovery, dryness risk, and long-term stability for each patient? LASIK and SMILE are both forms of refractive surgery, meaning procedures that change how the eye bends light so images focus more clearly on the retina. Both can reduce dependence on glasses or contact lenses, but they reach that goal in different ways: LASIK reshapes the cornea under a flap, while SMILE removes a tiny lens-shaped piece of tissue through a small incision. This difference matters because the cornea is not just a transparent window; it is a living, nerve-rich, biomechanical structure that affects clarity, comfort, and eye stability.
The Problem: Blurred Vision Starts With Imperfect Focusing
Myopia, hyperopia, and astigmatism are refractive errors, which means the eye’s focusing system does not place light exactly on the retina. In myopia, or nearsightedness, distant objects appear blurred; in hyperopia, or farsightedness, near vision is often more difficult; in astigmatism, irregular curvature of the cornea or lens distorts the image. Glasses and contact lenses compensate for these focusing errors from outside the eye, while refractive surgery changes the cornea itself so light bends more accurately. The FDA describes LASIK as a procedure in which controlled laser removal of corneal tissue reshapes the cornea and changes its focusing power. The key structure in both LASIK and SMILE is the corneal stroma, the middle layer of the cornea that provides much of its shape and strength. In clinical practice, the challenge is not simply removing tissue; it is removing the correct amount, in the correct location, while leaving enough healthy cornea behind. This matters because an over-treated, under-treated, or structurally weakened cornea can lead to poor vision quality, glare, halos, dry eye symptoms, or rare but serious complications such as corneal ectasia, where the cornea progressively bulges forward.







- Two procedures reshape the cornea to improve focusing.
- Laser-Assisted In Situ Keratomileusis (LASIK) uses a flap; Small Incision Lenticule Extraction (SMILE) uses a small incision.
- The best choice depends on the right eye.
How LASIK Works: A Flap, an Excimer Laser, and Fast Visual Recovery
LASIK stands for laser-assisted in situ keratomileusis, a term that means reshaping the cornea while preserving the outer surface as a flap. During LASIK, a surgeon creates a thin corneal flap using either a microkeratome blade or a femtosecond laser, lifts the flap, and then uses an excimer laser, a cool ultraviolet laser, to remove microscopic layers of stromal tissue. The flap is then repositioned. The practical advantage is speed: LASIK often gives rapid visual recovery because the surface layer is largely replaced rather than removed. The trade-off is that flap creation cuts more corneal nerves and creates flap-specific risks, including flap displacement, inflammation, or interface problems. LASIK is commonly used for myopia, hyperopia, and astigmatism, but it is not a universal solution. FDA patient guidance emphasizes that outcomes vary by prescription, corneal thickness, healing response, surgeon experience, and device type. Patients with unstable prescriptions, keratoconus, thin corneas, significant dry eye, active eye disease, or medical conditions that impair wound healing may not be suitable candidates. This matters because LASIK is elective surgery on healthy eyes, so patient selection is as important as the laser itself.
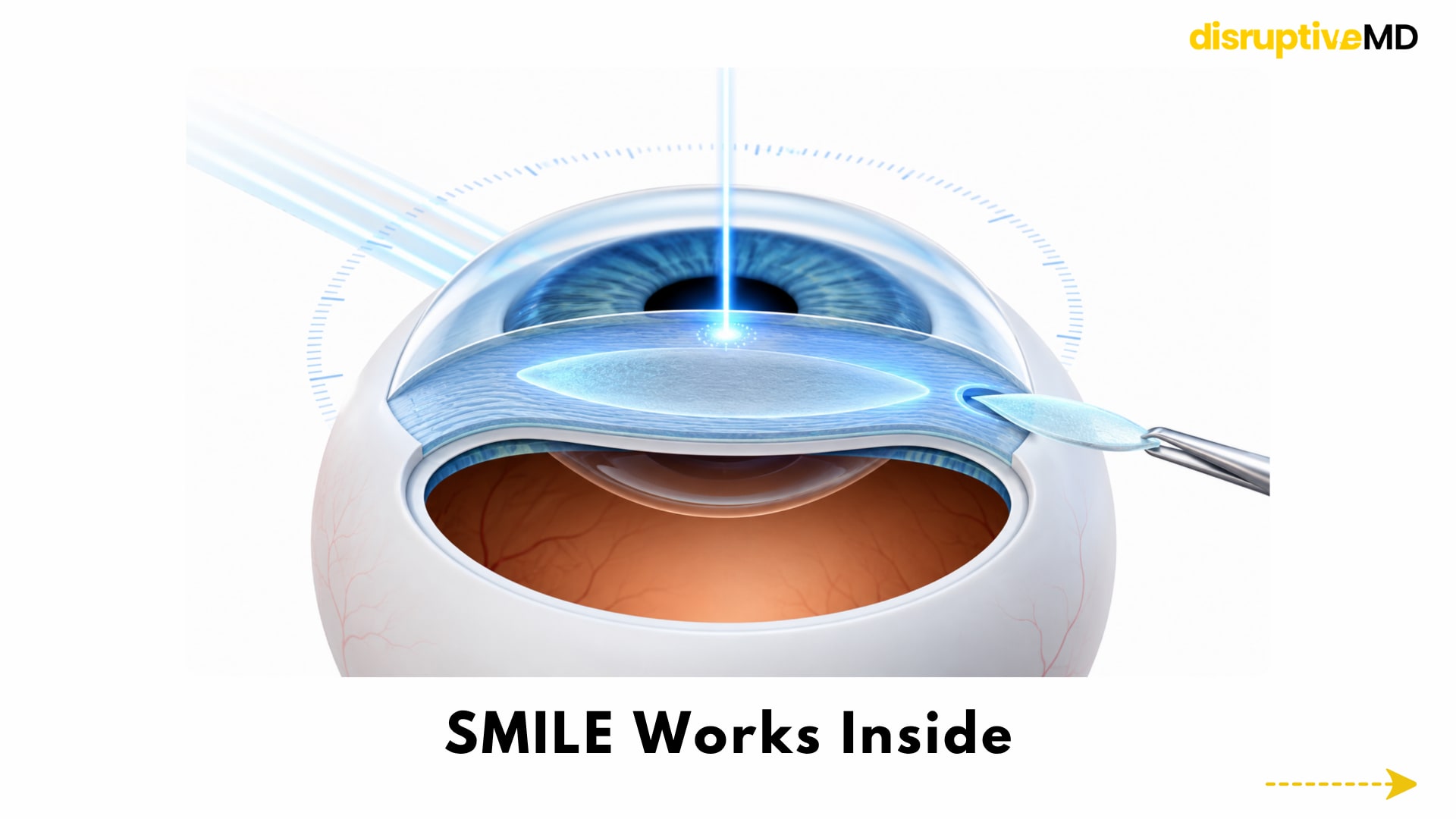
How SMILE Works: A Flapless Lenticule Extraction Procedure
SMILE stands for small incision lenticule extraction, a flapless laser procedure mainly used to treat myopia with or without astigmatism. Instead of lifting a flap, a femtosecond laser creates a thin disc-shaped piece of tissue inside the cornea called a lenticule; the surgeon then removes that lenticule through a small incision. Removing the lenticule changes the corneal shape and reduces the focusing error. The idea is elegant: reshape the cornea from within while disturbing less of the front corneal surface. SMILE’s biggest design difference is preservation of more anterior corneal tissue and potentially more of the corneal nerve network. The subbasal nerve plexus, a fine layer of corneal nerves near the surface, helps maintain corneal sensation and tear-film feedback; when these nerves are disrupted, dry eye symptoms can appear after surgery. Because SMILE does not require a large flap, studies and reviews suggest it may cause less early postoperative dry eye and less temporary reduction in corneal sensitivity than femtosecond LASIK, although the size and durability of this advantage vary between studies.
Evidence and Real-World Meaning: Two Different Paths to Clearer Vision
LASIK and SMILE both aim to solve the same everyday problem: blurred vision caused by the eye focusing light in the wrong place. The difference lies in how each procedure reaches that goal. LASIK works like opening a precise access door on the cornea, reshaping the inner tissue with a laser, and then placing the flap back in position. This approach has become familiar to many clinicians because it is versatile, widely practiced, and often associated with quick visual recovery. In real life, this means many patients notice clearer vision soon after surgery, although comfort, dryness, night vision, and healing can vary from person to person. SMILE takes a quieter and more minimal route. Instead of creating a flap, the laser forms a tiny lens-shaped layer of tissue inside the cornea, called a lenticule, which is removed through a small opening. Once this tissue is removed, the cornea changes shape and light focuses more accurately. The appeal of SMILE is that it keeps more of the corneal surface structure intact, which may be helpful for some patients who are concerned about dryness, corneal strength, or flap-related issues. In simple clinical terms, SMILE is often seen as a less surface-disruptive option, especially for suitable patients with myopia. The real-world difference between the two procedures is not that one is “good” and the other is “bad.” LASIK is often valued for its speed, flexibility, and long history of use, while SMILE is valued for its flapless design and smaller incision. LASIK may be preferred when a wider range of refractive errors needs correction or when future enhancement planning is important. SMILE may be preferred when the goal is to reduce flap-related concerns and preserve more of the corneal surface architecture. Both procedures depend heavily on careful screening, because the best result comes from matching the technique to the patient’s corneal thickness, prescription, tear-film health, lifestyle, and visual expectations. In clinical practice, the choice between SMILE and LASIK is less like choosing the “latest” procedure and more like choosing the right surgical design for the right eye. A patient with healthy corneas, stable vision, and good tear function may do well with either option. A patient with dry eye symptoms, thin corneal measurements, unusual corneal shape, or high visual demands may need more detailed evaluation before either surgery is considered. This matters because laser vision correction is not simply a cosmetic convenience; it is a permanent reshaping of a delicate optical structure. The most meaningful outcome is not only sharper vision, but comfortable, stable, and reliable vision in daily life.
Limitations, Risks, and Unanswered Questions
The main limitation of LASIK is that the flap is both its strength and its weakness. The flap helps explain fast recovery, but it also introduces flap-related risks and may disturb more corneal nerves, which can contribute to dry eye symptoms. FDA guidance lists possible LASIK risks including loss of lines of vision, glare, halos, double vision, undercorrection or overcorrection, severe dry eye, and reduced quality of vision in low-contrast settings such as night driving. These effects are not the norm for most well-screened patients, but they are clinically important because refractive surgery changes the eye permanently. The main limitation of SMILE is that flapless does not mean risk-free. FDA safety documents list possible SMILE-related adverse effects including undercorrection, overcorrection, dry eye, glare, halos, night-driving difficulty, inflammation, infection, difficult lenticule removal, retained lenticule tissue, and rare corneal complications. SMILE may also be less flexible than LASIK for certain prescriptions, especially hyperopia in many regulatory settings, and enhancement surgery after SMILE can be more technically complex because there is no existing LASIK flap to lift. This matters because the best procedure is not determined only by incision size; it depends on prescription, corneal shape, ocular surface health, visual goals, and the surgeon’s ability to manage complications. A major unanswered question is whether SMILE’s early advantages in dryness and corneal nerve preservation translate into consistently better long-term patient experience across diverse populations. Some studies show better early tear-film stability or corneal sensitivity after SMILE, while other analyses suggest differences may narrow over time. Researchers also continue to study higher-order aberrations, which are subtle optical distortions that can affect night vision, contrast, and visual sharpness even when standard vision-chart results look good. This matters because future refractive surgery success will be judged less by “20/20” alone and more by comfort, stability, visual quality, and long-term safety.
Conclusion
SMILE and LASIK are not competing slogans; they are two different engineering solutions to the same optical problem. LASIK uses a flap and an excimer laser to reshape the cornea with fast recovery and broad clinical use. SMILE uses a femtosecond laser to remove an internal lenticule through a small incision, avoiding a flap and potentially reducing early dry eye symptoms in selected patients. The most realistic conclusion is that both procedures can work well when the right patient, prescription, cornea, technology, and surgeon come together. For patients and clinicians, the future of refractive surgery is not about declaring one universal winner; it is about better screening, more transparent risk counseling, and more personalized procedure selection.
Evidence Rating
Regulatory-approved. LASIK laser systems and SMILE devices have regulatory pathways and approved indications, and both are supported by clinical studies and real-world ophthalmic use. However, the head-to-head comparison remains partly mixed, because final visual outcomes are often similar while differences in dry eye, visual quality, recovery speed, and suitability depend on patient selection, device platform, prescription range, and follow-up duration.
Educational Disclaimer
This article is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Decisions about LASIK, SMILE, or any refractive procedure should be made after a full eye examination and consultation with a qualified eye-care professional.
References
- U.S. Food and Drug Administration. What is LASIK?
- U.S. Food and Drug Administration. LASIK: Risks and Patient Information.
- U.S. Food and Drug Administration. FDA-Approved Lasers for LASIK / Patient Information.
- U.S. Food and Drug Administration. VisuMax Femtosecond Laser PMA Approval: SMILE for Myopia With or Without Astigmatism.
- U.S. Food and Drug Administration. Summary of Safety and Effectiveness Data: VisuMax SMILE.
- Hays RD, Tarver ME, Spritzer KL, et al. Assessment of the Psychometric Properties of a Questionnaire Assessing Patient-Reported Outcomes With LASIK (PROWL). JAMA Ophthalmology.
- U.S. Food and Drug Administration. LASIK Quality of Life Collaboration Project / PROWL Study Results.
- Chen KY, et al. Keratorefractive Lenticule Extraction Surgery Compared With LASIK for Dry Eye Outcomes: Systematic Review and Meta-analysis.
- Tsatsos M, Giachos I, Prousali E, Jacob S, Ziakas N. Is SMILE Ready to Become the Gold Standard in Laser Refractive Surgery? Eye