
What if osteoporosis treatment moved from “slowing bone loss” to rebuilding stronger, smarter, fracture-resistant bone?
Introduction
For many years, osteoporosis was described mainly as a silent disease of low bone density. A patient had a bone density scan, received a T-score, and treatment often focused on slowing further bone loss.
That view is changing.
Osteoporosis is now increasingly understood as a disease of bone strength, bone quality, ageing biology, hormones, muscle loss, fall risk, and fracture prediction. The real danger is the first fracture, a hip fracture, vertebral fracture, wrist fracture, or spine fracture that can change mobility, independence, confidence, and long-term health.
The future of osteoporosis care is moving from passive monitoring to active bone-risk engineering.
The new goal is not simply to “treat low bone density.” It is to identify high-risk patients earlier, rebuild bone where possible, sequence therapies intelligently, protect muscle and balance, prevent falls, and reduce fractures before they happen.




- Osteoporosis is now increasingly understood as a disease of bone strength, bone quality, ageing biology, hormones, muscle loss, fall risk, and fracture prediction.
- The real danger is not only a low number on a scan.
- The future of osteoporosis care is moving from passive monitoring to active bone-risk engineering.
Bone-Building Therapy: Moving Beyond “Slowing Bone Loss”
Traditional osteoporosis treatment has mainly focused on antiresorptive medicines. These are drugs that slow down the cells responsible for breaking down bone. This approach is still important. But for some patients, especially those at very high fracture risk, slowing bone loss may not be enough.
This is where osteoanabolic therapy becomes disruptive.
Osteoanabolic treatment means treatment that stimulates new bone formation. Instead of only telling the body to “stop losing bone,” these therapies help shift the system toward rebuilding bone. This changes the treatment philosophy from “Stop losing bone” to “Rebuild bone first, then protect the gains".
This is especially important for patients who already have recent fractures, multiple vertebral fractures, very low bone density, or fractures despite previous treatment. These patients do not just need long-term prevention. They may need rapid strengthening of a fragile skeleton.
Important bone-building therapies include teriparatide, abaloparatide, and romosozumab. Teriparatide and abaloparatide act through pathways related to parathyroid hormone signalling, which can stimulate bone formation. Romosozumab works differently by targeting sclerostin, a protein involved in controlling bone formation.
The disruptive idea is not that every patient should receive the newest drug. The breakthrough is patient selection.
Some patients may do well with standard antiresorptive therapy. Others, especially those at very high risk, may benefit from an anabolic-first strategy. In this model, treatment begins with a bone-building phase and is then followed by an antiresorptive medicine to maintain the bone gained.
That second step matters. Bone-building therapy is not usually a “one and done” solution. If the newly built bone is not protected afterward, the gains may fade. Osteoporosis care is therefore becoming less like prescribing a single drug and more like designing a treatment sequence.
Sclerostin Inhibition: Unlocking the Body’s Bone-Building Pathway
One of the most exciting shifts in osteoporosis treatment is the move toward mechanism-based therapy.
Sclerostin is a protein produced by osteocytes, the cells embedded inside bone. In simple terms, sclerostin acts like a brake on bone formation. When sclerostin activity is high, bone-building signals are reduced.
Sclerostin inhibitors work by blocking this brake.
Romosozumab is the best-known example. It is disruptive because it has a dual effect: it can increase bone formation and reduce bone resorption at the same time. This makes it different from older treatments that mainly focused on slowing bone breakdown.
This represents a major change in how we think about bone. Bone is not a passive mineral structure. It is living tissue. It constantly remodels, repairs, responds to hormones, reacts to mechanical load, and communicates through molecular signals. Sclerostin inhibition shows that osteoporosis treatment can target these signals directly.
Romosozumab is generally used for selected patients at high or very high fracture risk, not for every osteoporosis patient. It is usually given for a defined treatment period and then followed by an antiresorptive drug to maintain the improvement in bone density and fracture protection.
Cardiovascular safety screening is also important. Patients with a high risk of heart attack or stroke may not be suitable candidates, depending on their medical history and clinician assessment.
Smarter Sequencing: Osteoporosis Treatment as a Long-Term Strategy, Not a Single Drug
One of the biggest breakthroughs in osteoporosis care is not only the arrival of new drugs.
It is learning how to use them in the right order.
Osteoporosis is a long-term condition. A patient may move through different treatment phases over time:
First, rebuild bone if fracture risk is very high. Next, preserve the gains and prevent rebound bone loss. monitor fracture risk and bone density. Thereafter, adjust treatment as age, health, falls risk, and fracture history change. This is why treatment sequencing matters.
For example, a very high-risk patient may start with anabolic therapy and then switch to an antiresorptive medicine. This helps preserve the bone gained during the rebuilding phase.
Denosumab is another example where planning matters. It can be highly effective, but it should not be stopped suddenly without another appropriate treatment plan.* When denosumab is delayed or stopped without follow-up therapy, bone turnover can rebound, bone density can fall quickly, and fracture risk may rise*.
This is also why the idea of a “drug holiday” needs to be understood carefully. Drug holidays are mainly discussed with certain bisphosphonates in selected lower-risk patients after reassessment. They do not apply to every osteoporosis medicine.
AI and Precision Fracture-Risk Prediction
A major problem in osteoporosis is that many people are diagnosed only after they fracture.
The future of osteoporosis treatment may begin before the patient even knows they have osteoporosis.
AI and advanced imaging could help detect silent bone loss and hidden vertebral fractures earlier. One of the most interesting ideas is opportunistic screening.
A patient may undergo a CT scan of the chest, abdomen, spine, or another body part for an unrelated reason. In the future, AI tools may be able to analyse that scan in the background and flag signs of low bone density, vertebral compression fractures, or abnormal bone quality. This could turn routine medical imaging into an early-warning system for fracture risk.
DXA (Dual-Energy X-ray Absorptiometry) remains a central tool for measuring bone mineral density.
But bone density is not the whole story. Fracture risk also depends on bone architecture, trabecular structure, microdamage, falls, muscle strength, vision, balance, medications, and overall health.
This is where tools such as trabecular bone score become interesting.
Trabecular bone score uses information from lumbar spine DXA images to provide insight into bone microarchitecture. It does not replace DXA, but it may add another layer of fracture-risk information.
FRAX (Fracture Risk Assessment Tool) is already used to estimate fracture probability based on clinical risk factors, with or without bone density.
In the future, fracture-risk tools may become more intelligent by combining age, fracture history, medications, imaging data, bone quality markers, muscle measures, fall risk, and AI-derived scan features.
The important limitation is that AI must be validated properly. It must work across different scanners, populations, hospitals, and workflows. It must support clinicians, not replace clinical judgement.
Regenerative, Cellular, and Next-Generation Bone Medicine
The most futuristic area of osteoporosis treatment is the attempt to move beyond current drugs and target deeper skeletal biology.
Osteoporosis is strongly linked with ageing. As the body ages, bone-forming cells become less active, bone-resorbing activity may dominate, hormones change, inflammation increases, muscle mass declines, and the bone-remodelling environment becomes less efficient.
This means osteoporosis is not only a bone-density problem. It is a disorder of the entire bone-remodelling ecosystem.
Researchers are exploring stem cell biology, exosome-based therapies, senescent cells, osteoimmunology, mitochondrial dysfunction, Wnt pathway signalling, targeted drug delivery, and next-generation anabolic agents.
Exosomes are tiny extracellular vesicles released by cells. They can carry biological messages between cells and may one day be used to influence bone repair, inflammation, regeneration, or drug delivery.
At present, this is still largely experimental for osteoporosis and should not be presented as routine clinical care.
Stem cell ageing is another major area of interest.
Mesenchymal stem cells can help generate bone-forming cells, but with ageing, their regenerative potential may decline.
Research is exploring whether improving the function of these cells could support bone formation and skeletal repair.
Osteoimmunology is also important. This field studies the relationship between the immune system and bone.
Chronic inflammation can influence bone loss, and immune signals can affect both bone-forming and bone-resorbing cells.
Then there is the muscle-bone connection.
Muscle is not just for movement. Strong muscle helps protect bone by improving balance, reducing falls, and mechanically stimulating bone.
This is why sarcopenia and osteoporosis are so closely linked. Weak bone plus weak muscle is a dangerous combination.
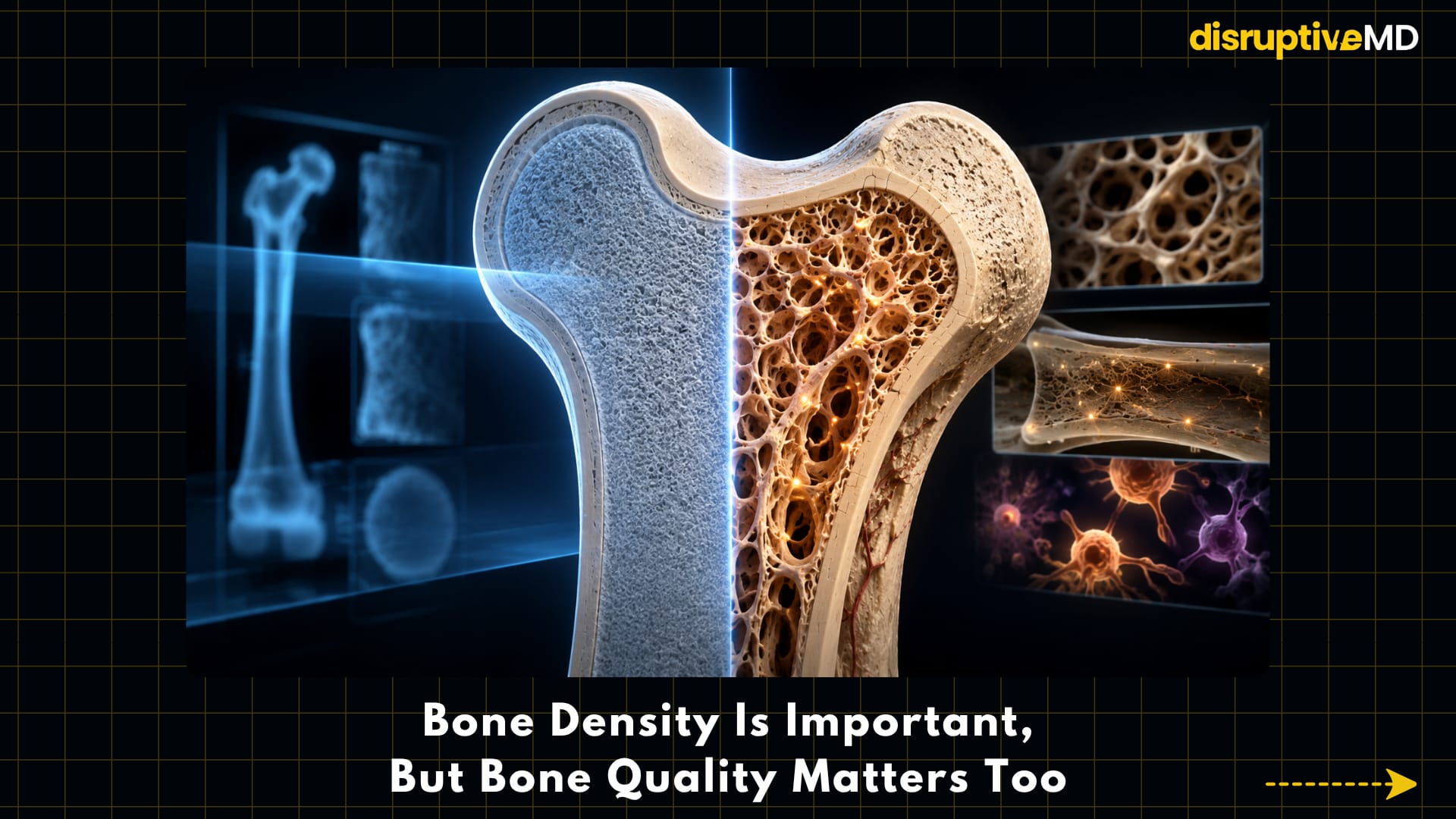
Bone Density Is Important, But Bone Quality Matters Too
A DXA scan is important because it measures bone mineral density. But fracture risk is more complex than a single number. T wo people may have similar bone density scores but different fracture risks.
Why?
Because bone strength depends on more than mineral content. It also depends on bone architecture, trabecular structure, cortical thickness, microdamage, turnover rate, age, prior fractures, medications, balance, vision, muscle strength, and fall risk.
This is why the future of osteoporosis care must look beyond “What is the T-score?”
It must ask:
- How strong is the bone?
- How likely is the patient to fall?
- Has the patient already fractured?
- Is there hidden vertebral fracture?
- Is muscle loss present?
- Are medications increasing fall risk?
- Is treatment being monitored?
- Is the patient at high risk now, or very high risk now?
Osteoporosis is not just a scan result. It is a fracture-risk condition.
Falls Are Part of Osteoporosis Treatment
A person does not fracture only because the bone is weak.
A person often fractures because weak bone meets a fall.
That means fall prevention is not optional. It is part of osteoporosis treatment.
Future bone health care must include strength training, balance training, gait assessment, vision correction, medication review, home safety, footwear assessment, vitamin D optimisation where needed, and fall-risk prediction.
This is where osteoporosis overlaps with orthopaedics, endocrinology, physiotherapy, geriatrics, sports science, rehabilitation, and longevity medicine.
A stronger skeleton matters. But so does the ability to stay upright, stable, coordinated, and mobile.
The Treatment Gap: The Missed Opportunity After a Fracture
One of the biggest failures in osteoporosis care is not a lack of drugs. It is a failure to act after a fracture.
Many patients who suffer a fragility fracture are treated for the broken bone but are not properly evaluated or treated for the disease that made the fracture more likely in the first place.
This is where fracture liaison services become disruptive.
A fracture liaison service is an organised system that identifies patients with fragility fractures, assesses osteoporosis risk, starts appropriate treatment, and ensures follow-up. It closes the gap between fracture care and fracture prevention.
This may not sound as futuristic as AI or regenerative medicine. But it may be one of the most powerful innovations in real-world osteoporosis care.
Preventing the second fracture begins when the first fracture happens.
Fact Base
Osteoporosis treatment is moving from a narrow focus on bone density toward a broader model of fracture-risk reduction.
Bone-building medicines such as teriparatide, abaloparatide, and romosozumab are especially important for selected patients at very high fracture risk.
Romosozumab targets sclerostin, a protein that acts as a brake on bone formation and has a dual effect on bone formation and resorption.
Treatment sequencing matters. Bone-building therapy is usually followed by antiresorptive therapy to preserve gains.
Denosumab should not be stopped suddenly without a follow-up treatment plan because rebound bone turnover and bone loss can occur.
Bisphosphonate drug holidays may be considered only in selected patients after reassessment and do not apply to every osteoporosis medicine.
DXA remains central, but fracture risk also depends on bone quality, vertebral fractures, muscle strength, falls, medications, age, and prior fractures.
AI-assisted imaging may help detect low bone density or vertebral fractures from scans performed for other medical reasons, but these tools require validation and workflow integration.
Fracture liaison services are important because many patients remain untreated even after fragility fractures.
Regenerative and cellular approaches such as exosome-based therapy, stem-cell biology, senescence targeting, and bone-targeted delivery are promising research areas but are not routine clinical osteoporosis treatment yet.
Important Limitations
Osteoporosis treatment is improving, but there is no single perfect therapy.
Not every patient needs the newest treatment. Some therapies are reserved for very high-risk patients. Some drugs have time limits. Some have important safety considerations. Cost and access matter. Treatment transitions must be planned. Calcium, vitamin D, protein, exercise, strength training, and fall prevention still matter.
Future regenerative treatments are exciting, but they should be presented honestly: promising, experimental, and not yet standard care for routine osteoporosis treatment.
The future is not about replacing basic bone health. It is about combining basic bone health with smarter drugs, better sequencing, earlier detection, stronger muscles, safer movement, and more personalised risk prediction.
Final Takeaway
Osteoporosis treatment is entering a new era.
The future is not just about increasing a number on a bone density scan. It is about predicting fracture risk earlier, rebuilding bone in the right patients, sequencing therapies intelligently, protecting muscle and balance, preventing falls, closing the treatment gap, and eventually targeting the biology of skeletal ageing itself.
The next breakthrough in osteoporosis may not be a stronger pill. It may be a smarter, personalised strategy to keep bones strong before they break.
References:
-
Eastell R, Rosen CJ, Black DM, et al. Pharmacological Management of Osteoporosis in Postmenopausal Women: An Endocrine Society Clinical Practice Guideline. Journal of Clinical Endocrinology & Metabolism.2019;104(5):1595–1622. DOI: https://doi.org/10.1210/jc.2019-00221
-
Shoback D, Rosen CJ, Black DM, et al. Pharmacological Management of Osteoporosis in Postmenopausal Women: An Endocrine Society Guideline Update. Journal of Clinical Endocrinology & Metabolism.2020;105(3):dgaa048. DOI: https://doi.org/10.1210/clinem/dgaa048.
-
National Osteoporosis Guideline Group — Summary of Main Recommendations. Updated September 2024. Link: https://www.nogg.org.uk/full-guideline/summary-main-recommendations
-
National Osteoporosis Guideline Group — Pharmacological Treatment Options. Updated 2024. Link: https://www.nogg.org.uk/full-guideline/section-6-pharmacological-treatment-options.
-
Neer RM, Arnaud CD, Zanchetta JR, et al. Effect of Parathyroid Hormone 1-34 on Fractures and Bone Mineral Density in Postmenopausal Women with Osteoporosis. New England Journal of Medicine.2001;344:1434–1441. DOI: https://doi.org/10.1056/NEJM200105103441904
-
Miller PD, Hattersley G, Riis BJ, et al. Effect of Abaloparatide vs Placebo on New Vertebral Fractures in Postmenopausal Women With Osteoporosis: A Randomized Clinical Trial. JAMA. 2016;316(7):722–733. DOI: https://doi.org/10.1001/jama.2016.11136
-
Cosman F, Crittenden DB, Adachi JD, et al. Romosozumab Treatment in Postmenopausal Women with Osteoporosis. New England Journal of Medicine. 2016;375:1532–1543. DOI: https://doi.org/10.1056/NEJMoa1607948
-
Saag KG, Petersen J, Brandi ML, et al. Romosozumab or Alendronate for Fracture Prevention in Women with Osteoporosis. New England Journal of Medicine. 2017;377:1417–1427. DOI: https://doi.org/10.1056/NEJMoa1708322
-
Krupa KN, Parmar M. Romosozumab. StatPearls. NCBI Bookshelf. Updated 2024. Link: https://www.ncbi.nlm.nih.gov/books/NBK585139/
-
Engelke K, Museyko O, Wang L, Laredo JD. Opportunistic Screening Techniques for Analysis of CT Scans.Current Osteoporosis Reports. 2023. DOI: https://doi.org/10.1007/s11914-022-00764-5
-
International Osteoporosis Foundation — Other Diagnostic Tools: Trabecular Bone Score. Link: https://www.osteoporosis.foundation/health-professionals/diagnosis/other-diagnostic-tools
-
FRAXplus / FRAX fracture-risk tool. Link: https://www.fraxplus.org/
-
International Osteoporosis Foundation — Models of Care: Fracture Liaison Services. Link: https://www.osteoporosis.foundation/health-professionals/fragility-fractures/models-of-care
-
Miclau T, et al. Secondary fracture prevention: global approaches. OTA International. 2022. Link: https://pmc.ncbi.nlm.nih.gov/articles/PMC9359005/
-
Fang F, Li Z, et al. The role and applications of extracellular vesicles in osteoporosis. Bone Research. 2024. DOI: https://doi.org/10.1038/s41413-023-00313-5
-
Li K, Hu S, Chen H. Cellular senescence and other age-related mechanisms in skeletal diseases. Bone Research. 2025;13:68. DOI: https://doi.org/10.1038/s41413-025-00448-7
-
Targeting Crosstalk of Signaling Pathways among Muscles-Bone-Adipose Tissue: A Promising Therapeutic Approach for Sarcopenia. Aging and Disease. 2024;15(4):1619–1645. DOI: https://doi.org/10.14336/AD.2023.00903