
What if rehabilitation could build strength before the body is ready for heavy loading?
Rehabilitation is no longer just about doing exercises, waiting for time to pass, and slowly returning to activity.
The next era of rehab is becoming more measurable, personalised, and biologically intelligent.
Traditionally, rehabilitation was built around rest, mobility, strengthening, balance, pain control, and gradual return to function. Those foundations still matter. But modern recovery is now being supported by tools that can stimulate muscle, measure movement, guide loading, improve motor control, and protect healing tissues while the patient rebuilds strength.
Blood flow restriction (BFR) training, neuromuscular electrical stimulation (NMES), electromyographic (EMG) biofeedback, wearable sensors, force plates, smart insoles, video-based movement analysis, virtual reality, and AI-guided rehabilitation are changing how recovery is monitored and progressed.
The goal is not to replace the physiotherapist, surgeon, trainer, or rehabilitation specialist.
The goal is to give them better information.
The future of rehab is not just doing more exercises. It is knowing what the body is ready for, what the muscle is actually doing, how the nervous system is controlling movement, and when the patient can safely progress.




- The body needs strength.
- But the healing tissue cannot tolerate heavy loading yet.
- How do we stimulate muscle, restore control, and rebuild capacity without overloading healing tissue too early?
The Rehab Paradox
Many injuries and surgeries create the same problem: The body needs strength, but the healing tissue cannot tolerate heavy loading yet.
This is common after ACL reconstruction, meniscus repair, rotator cuff repair, tendon injury, fracture surgery, cartilage repair, joint replacement, immobilisation, muscle injury, chronic pain, and neurological injury.
The patient needs to rebuild capacity, but the repaired tissue may still need protection. The muscle needs stimulation, but the joint may still be swollen. The nervous system needs control, but pain or fear may be changing movement.
This creates the central rehab paradox: How do we stimulate muscle, restore control, and rebuild capacity without overloading healing tissue too early?
That is where BFR, neuromuscular technology, sensors, and AI become disruptive.
From Time-Based Rehab to Readiness-Based Rehab
Old rehab often depended heavily on time-based protocols.
Week 2: do this.
Week 6: start that.
Month 3: progress here.
Time still matters because biology needs time to heal. But time alone is not enough.
Two patients may be at the same stage after surgery but have completely different strength, swelling, pain, confidence, muscle activation, walking quality, and movement control.
Modern rehab is moving toward criteria-based progression. That means decisions are based on readiness, not just the calendar. Readiness may include strength, pain, swelling, range of motion, gait, balance, movement quality, muscle activation, tissue healing stage, functional performance, fatigue response, and sport-specific control.
The future is not simply: “How many weeks since injury?” The future is: “What is the body ready for today?”
Blood Flow Restriction Training: Low Load, High Signal
Blood flow restriction training, or BFR, uses a specialised cuff placed around a limb to partially restrict blood flow during low-load exercise.
The patient may perform light exercise, but the muscle experiences a stronger internal metabolic stimulus than the external load would normally produce.
This is why BFR is so interesting in early rehabilitation.
Traditional strength training often requires heavier loads to stimulate muscle growth and strength. But after injury or surgery, heavy loading may be painful, unsafe, or too stressful for healing tissue.
BFR offers a different strategy: Low external load, high internal muscle stimulus.
It may help selected patients train muscle when heavy weights are not yet appropriate. This can be useful in ACL rehabilitation, knee surgery recovery, muscle atrophy prevention, joint replacement rehab, tendon rehabilitation, post-fracture weakness, cartilage repair protection, and return-to-sport progression.
But BFR is not just “tie a band around the limb.” Real BFR requires proper cuffs, correct pressure, screening, supervision, and clinical reasoning. Cuff pressure should be individualised based on limb size, cuff width, blood pressure, tissue tolerance, exercise type, rehab stage, training goal, and medical history.
BFR is promising, but it is not for everyone. Caution is important in people with blood clot history, vascular disease, uncontrolled hypertension, certain cardiac conditions, poor circulation, nerve symptoms, pregnancy considerations, high-risk medical status, or improper cuff use.
BFR is not a casual gym hack. It is a clinical and performance tool that must be dosed intelligently.
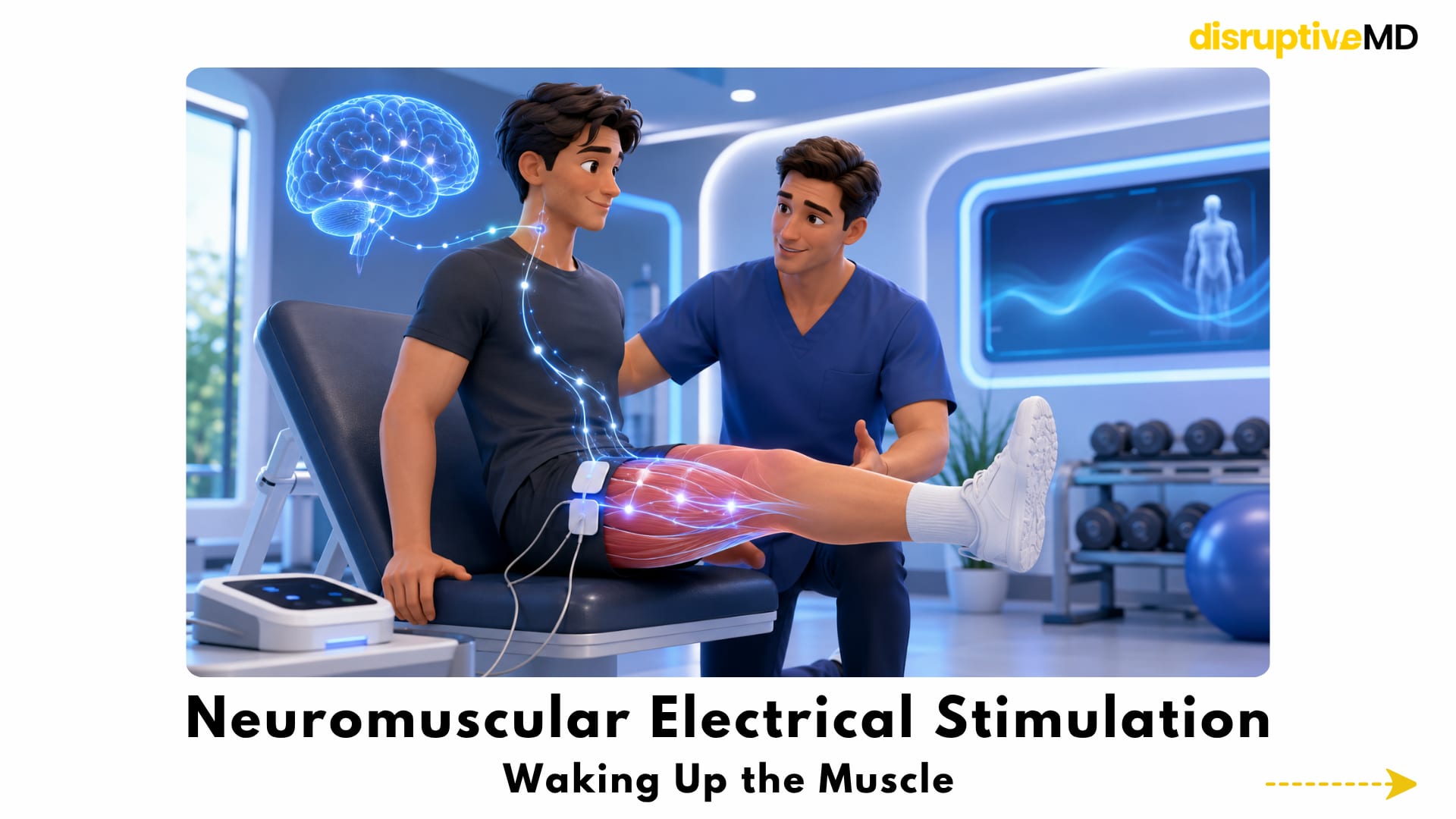
Neuromuscular Electrical Stimulation: Waking Up the Muscle
Neuromuscular electrical stimulation, or NMES, uses electrical impulses to activate muscles.
It is especially useful when the brain has difficulty fully activating a muscle after pain, swelling, injury, or surgery.
This is common after knee injuries and ACL reconstruction, where the quadriceps can “switch off.” The muscle may not be torn, but the nervous system may reduce activation as a protective response. This can lead to weakness, poor control, altered walking, delayed strength recovery, compensations, reduced return-to-sport readiness, and higher risk of poor movement patterns.
NMES can help externally stimulate contraction while the patient rebuilds voluntary control.
This is especially important for the quadriceps after knee injury and surgery because quadriceps strength affects walking, stairs, jumping, landing, cutting, deceleration, knee stability, and return to sport. NMES does not replace strength training. It helps rebuild the connection between the nervous system and the muscle so strength training can become more effective.
EMG Biofeedback: Seeing the Muscle Work EMG biofeedback measures muscle activation and shows the patient whether the right muscle is working.
This matters because a patient may think they are activating a muscle correctly, but another muscle may be compensating.
For example, a patient after ACL surgery may struggle to properly activate the quadriceps. A hip rehab patient may think they are using the glutes, but the hamstrings or lower back may dominate. A shoulder patient may need better scapular control. A post-stroke patient may need to relearn motor patterns.
EMG biofeedback makes invisible muscle activity visible. That changes rehab from guessing into feedback-based learning. When patients can see muscle activation, they can learn to control it more effectively.
This is one of the biggest shifts in modern rehab: the patient is no longer only told what to feel. They can see what the muscle is doing.
Wearables, Smart Insoles and Force Plates
Rehab does not only happen inside the clinic.
Patients walk, climb stairs, sit, stand, sleep, compensate, avoid load, and return to daily life outside the appointment.
Wearable sensors can track movement beyond the clinic. They may measure steps, joint motion, gait symmetry, activity levels, walking speed, sleep, recovery trends, exercise adherence, and return-to-sport workload.
Smart insoles and force plates can measure how the patient loads each limb.
This matters because patients often unconsciously protect the injured side. They may walk, squat, jump, or land asymmetrically even when they feel “normal.”
Force data can reveal hidden deficits.
A patient may regain strength but still move poorly. That is why future rehab must measure not only strength, but also landing mechanics, knee valgus, hip control, trunk control, balance, deceleration, cutting mechanics, asymmetry, fatigue response, and coordination.
This is especially important in athletes. Returning to sport is not just about being healed. It is about being ready to move under pressure, fatigue, speed, and unpredictability.
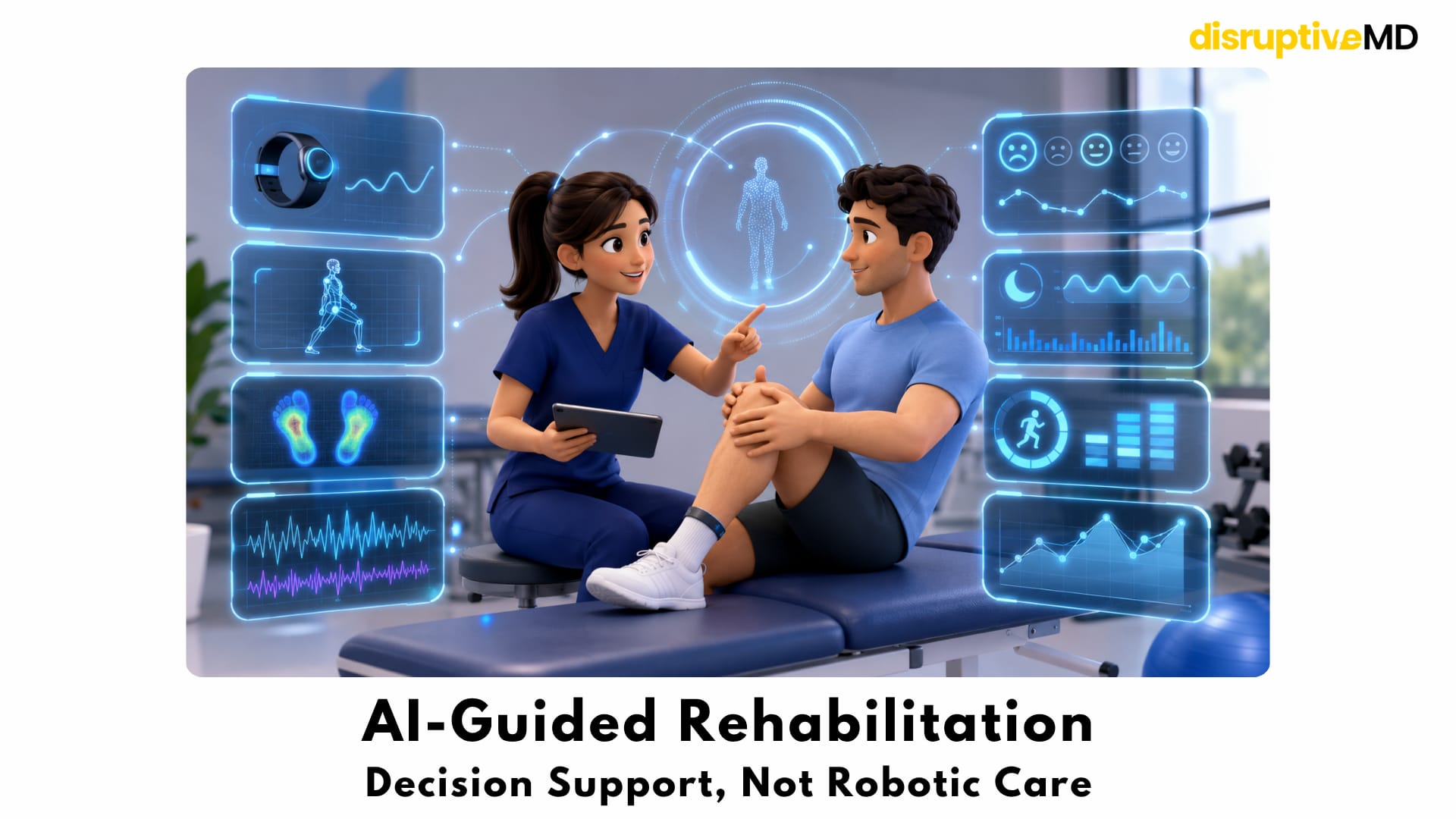
AI-Guided Rehabilitation: Decision Support, Not Robotic Care
AI may become one of the most powerful tools in rehabilitation, but only if it is used responsibly.
AI can help analyse data from wearables, video movement, force plates, EMG, pain logs, sleep patterns, patient-reported outcomes, and training workload.
It may help identify who is progressing well, who is underloading, who is overloading, who is compensating, who may be at risk of reinjury, and when rehab needs adjustment.
But AI should not replace clinicians.
Rehabilitation is too human and too complex for robotic decision-making. Pain, fear, motivation, sleep, tissue healing, surgical details, sport demands, life stress, and confidence all matter.
The goal of AI is clinical decision support. AI can help organise data. The clinician still makes the decision.
The future is not AI instead of physiotherapists. The future is physiotherapists, surgeons, trainers, and rehab specialists using better data to guide better recovery.
Video Analysis, VR and Robotic Rehab
Computer vision can analyse movement from camera footage.
This may support remote or clinic-based assessment of squat mechanics, gait, jump landing, shoulder motion, spinal posture, balance tasks, exercise technique, and compensations.
Virtual reality can turn rehab into an interactive training environment. It may help with balance, coordination, reaction time, post-stroke recovery, sports decision-making, fear of movement, pain distraction, engagement, and adherence.
The value is not just entertainment.
It is controlled, measurable, repeatable motor learning.
Robotic-assisted rehab and exoskeletons are especially relevant in neurological rehabilitation, spinal cord injury, stroke recovery, gait retraining, and severe weakness. These tools can support repeated, guided movement when patients cannot perform enough repetitions independently.
Brain-computer interface rehab goes even deeper. In the future, brain signals may be connected with external feedback, stimulation, robotics, or movement practice to help retrain motor pathways after neurological injury.
This is still highly specialised, but it represents one of the deepest frontiers of rehabilitation.
Closed-Loop Rehab: The Intelligent Recovery System
The most futuristic idea in rehab is closed-loop rehabilitation.
Closed-loop rehab means the system measures performance and adjusts the intervention in real time.
If muscle activation is low, stimulation may increase.
If gait becomes asymmetric, feedback may appear.
If loading is too high, exercise difficulty may drop.
If movement quality improves, the system may progress the task.
If fatigue changes mechanics, the system may flag the risk.
This is the future of intelligent rehab: Measure. Adapt. Stimulate. Teach. Progress.
A fixed protocol cannot do that. A smart rehab system can move closer to it.
Rehab After Surgery and Orthobiologics
Surgery repairs structure.
Rehab restores function.
A repaired ACL, meniscus, tendon, cartilage surface, fracture, or rotator cuff may be structurally healing, but the patient may still lack strength, control, endurance, confidence, mobility, proprioception, and sport-specific readiness.
This is why “healed” is not the same as “ready.”
Technology can help track the gap between structural recovery and functional recovery.
The same idea applies after orthobiologic treatments such as PRP or BMAC. These treatments are often discussed as injections, but recovery still depends on loading, movement quality, strength, and tissue-specific rehab.
The future may combine biologic treatment, BFR, sensor tracking, strength testing, movement retraining, and AI-guided progression.
That creates a more complete regenerative rehab model.
Not just inject and wait. Not just exercise and hope. But biology plus intelligent loading.
The Danger of Over-Technology
Technology does not automatically improve rehabilitation.
A bad rehab plan with expensive devices is still a bad rehab plan.
BFR does not replace progressive strength training.
NMES does not replace voluntary control.
Wearables do not replace clinical reasoning.
AI does not replace human judgement.
VR does not replace real-world function.
Force plates do not replace skilled movement analysis.
The essentials still matter: diagnosis, clinical reasoning, progressive loading, patient education, pain management, sleep, nutrition, consistency, recovery monitoring, and skilled supervision.
Technology should amplify good rehab. It should not decorate poor rehab.
Fact Base
BFR can provide a low-load muscle stimulus in selected patients when heavy loading is not yet appropriate.
BFR should be individualised using proper cuffs, appropriate pressure, medical screening, and supervision.
BFR is not universally safe and should not be treated as a casual gym hack.
NMES can support muscle activation when voluntary contraction is poor, especially after knee injury or ACL reconstruction.
EMG biofeedback can help patients understand whether the correct muscle is activating.
Wearables can track movement, activity, workload, sleep, and recovery patterns outside the clinic.
Smart insoles and force plates can reveal hidden loading asymmetry.
Video-based analysis and AI are emerging tools for movement assessment and rehab decision support.
VR and gamified rehab may improve engagement, repetition, feedback, and motor learning.
Robotic rehab and exoskeletons are most relevant in neurological rehabilitation, severe weakness, gait retraining, and high-repetition motor practice.
Return-to-sport decisions should not be based only on time. Strength, symmetry, movement quality, fatigue response, psychological readiness, and sport-specific capacity all matter.
AI-guided rehab is not robotic care. It is clinical decision support.
What Is Possible Today
- BFR can help create a low-load strength stimulus in selected patients.
- NMES can help when muscles are difficult to activate.
- EMG biofeedback can improve awareness and motor control.
- Wearables can monitor movement outside the clinic.
- Force plates and smart insoles can reveal asymmetry.
- Video analysis and AI are emerging tools for movement assessment.
- Rehab is becoming more measurable and criteria-based.
What is not fully possible yet:
- AI replacing physiotherapists.
- Wearables perfectly predicting injury risk.
- BFR working for every patient.
- NMES replacing strength training.
- One device solving all recovery problems.
- Remote rehab working without proper supervision.
- Return-to-sport clearance based on a single metric.
This balance is important. The future of rehab is exciting, but it must stay clinically honest.
Final Takeaway
The future of rehabilitation is not passive recovery.
It is precision recovery.
Blood flow restriction, neuromuscular stimulation, EMG biofeedback, wearable sensors, force data, video analysis, virtual reality, robotics, and AI are turning rehab into a measurable system that can protect healing tissue while rebuilding strength, control, and confidence.
The next revolution in recovery may not happen in the operating room. It may happen in the rehab lab.
References
- Patterson SD, Hughes L, Warmington S, Burr J, Scott BR, Owens J, et al. Blood Flow Restriction Exercise: Considerations of Methodology, Application, and Safety. Frontiers in Physiology. 2019. https://doi.org/10.3389/fphys.2019.00533
- Hughes L, Paton B, Rosenblatt B, Gissane C, Patterson SD. Blood Flow Restriction Training in Clinical Musculoskeletal Rehabilitation: A Systematic Review and Meta-analysis. British Journal of Sports Medicine. 2017. https://doi.org/10.1136/bjsports-2016-097071
- Cognetti DJ, Sheean AJ, Owens JG. Blood Flow Restriction Therapy and Its Use for Rehabilitation and Return to Sport. Arthroscopy, Sports Medicine, and Rehabilitation. 2022. https://doi.org/10.1016/j.asmr.2021.09.025
- Rice DA, McNair PJ. Quadriceps Arthrogenic Muscle Inhibition: Neural Mechanisms and Treatment Perspectives. Seminars in Arthritis and Rheumatism. 2010. https://doi.org/10.1016/j.semarthrit.2009.10.001
- Giggins OM, Persson UM, Caulfield B. Biofeedback in Rehabilitation. Journal of NeuroEngineering and Rehabilitation. 2013. https://doi.org/10.1186/1743-0003-10-60
- Porciuncula F, Roto AV, Kumar D, Davis I, Roy S, Walsh CJ, et al. Wearable Movement Sensors for Rehabilitation. PM&R. 2018. https://doi.org/10.1016/j.pmrj.2018.06.013
- Ardern CL, Glasgow P, Schneiders A, Witvrouw E, Clarsen B, Cools A, et al. 2016 Consensus Statement on Return to Sport. British Journal of Sports Medicine. 2016. https://doi.org/10.1136/bjsports-2016-096278
- Rutkowski S, Kiper P, Cacciante L, Cieślik B, Mazurek J, Turolla A, et al. Use of Virtual Reality-Based Training in Rehabilitation. Journal of Rehabilitation Medicine. 2020. https://doi.org/10.2340/16501977-2755
- Mehrholz J, Thomas S, Kugler J, Pohl M, Elsner B. Electromechanical-Assisted Training for Walking After Stroke. Cochrane Database of Systematic Reviews. 2020. https://doi.org/10.1002/14651858.CD006185.pub5
- Cervera MA, Soekadar SR, Ushiba J, Millán JDR, Liu M, Birbaumer N, Garipelli G. Brain-Computer Interfaces for Post-Stroke Motor Rehabilitation: A Meta-analysis. Annals of Clinical and Translational Neurology. 2018. https://doi.org/10.1002/acn3.544