
Introduction
A changing mole, photographed on a smartphone, may be evaluated by AI in seconds. But the main medical question is not whether software can find patterns. The key question is whether an AI system can reliably identify skin lesions that could be melanoma, basal cell carcinoma or squamous cell carcinoma, without giving false reassurance, costly operations, or missing cancers. Skin cancer is common and melanoma is the leading cause of skin cancer death. Early diagnosis often provides patients with more therapy alternatives. This is why dermatology AI on phones has gained actual clinical attention, especially in areas where access to dermatologists is limited.
The complex answer is that a phone could help catch and analyse a skin lesion, but it cannot diagnose skin cancer on its own way a biopsy can. Biopsy is still the gold standard for cancer confirmation. That means using a small piece of the suspect tissue and looking at it under a microscope. Today’s AI technologies are best thought of as decision-support systems that may help a clinician or patient decide whether a lesion needs to be evaluated by a medical professional, but they should not replace a dermatologist, clinical examination, dermoscopy or histopathology.
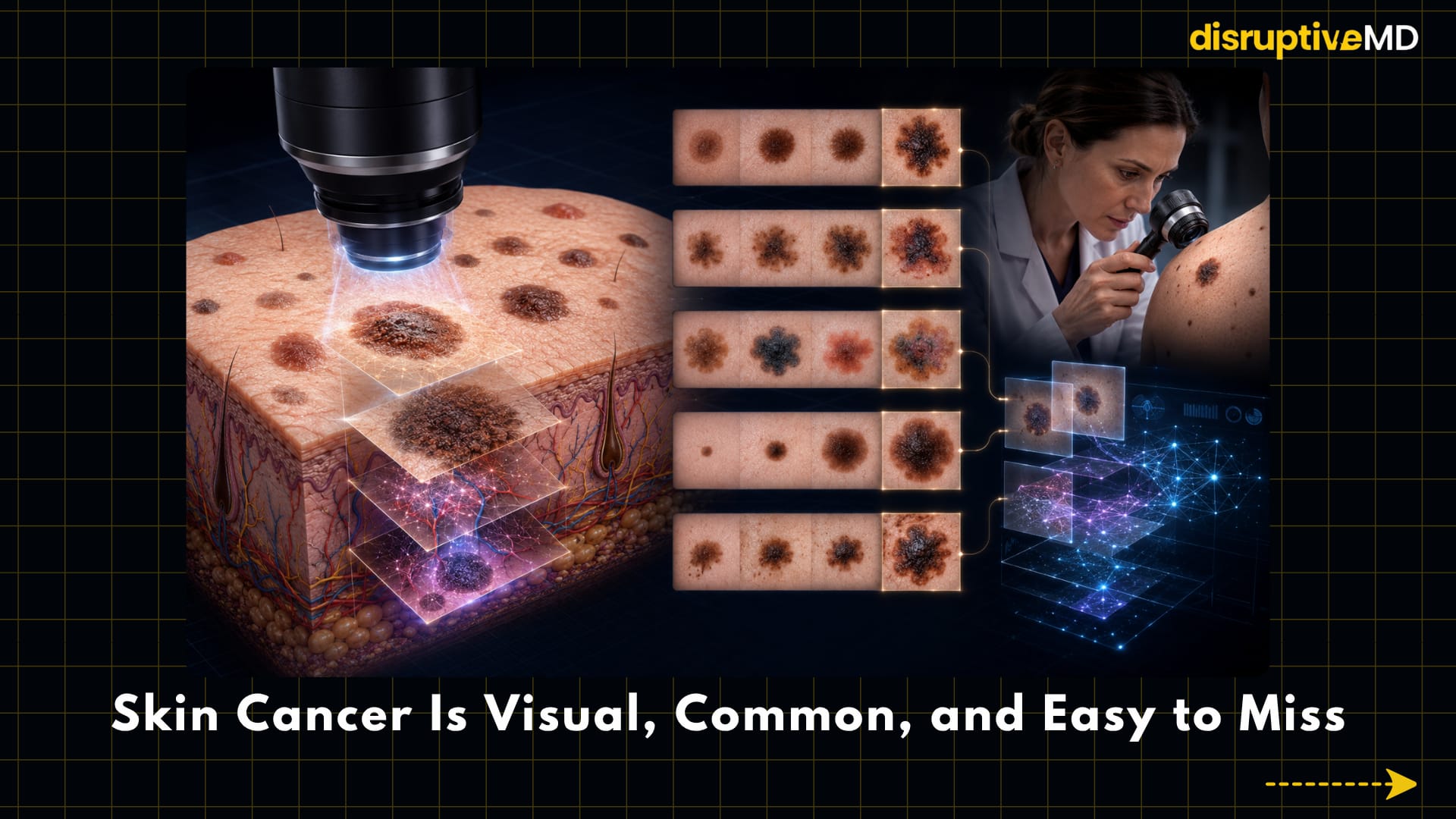
The Clinical Problem: Skin Cancer Is Visual, Common, and Easy to Miss
Most skin cancers begin with a change you can see on your skin. But that does not mean they are simpler to find. Melanoma is caused by abnormal cells in the skin that produce pigment. If melanoma is not detected early, it can spread. It is significantly more prevalent, and less lethal in many cases, but can cause harm to local tissue and requires treatment. Basal cell carcinoma and squamous cell carcinoma are collectively termed as keratinocyte carcinomas because they arise from the keratin-producing skin cells. This is crucial since the first sign of it is usually a lesion that looks a little odd, it changes over time, bleeds, grows or does not heal.
Clinicians commonly use visual principles such as ABCDE (asymmetry, border irregularity, colour variation, diameter, and evolution). Evolution is change over time and is often the most important warning signs. Another useful concept is the “ugly duckling” sign: one mole looks different to the patient’s other moles. These techniques are beneficial but are dependent on training, clinical experience, illumination, imaging quality, skin tone, location of the lesion and availability of the full patient history.
Dermoscopy is a technique that uses magnifying optical equipment to show subsurface patterns not easily seen by the human eye and improves this approach. Dermoscopy is a method used by dermatologists to examine pigment network, vascular pattern and lesion structures but still needs an expert interpretation. In fact, many suspicious lesions are first discovered in general care, urgent care, pharmacies, or through patient self-examination, when professional level dermoscopic assessment may not be available. This is the gap that AI dermatological technologies are trying to bridge.



- A changing mole, photographed on a smartphone, may be evaluated by AI in seconds.
- A phone could help catch and analyse a skin lesion, but it can’t diagnose skin cancer on its own.
- Biopsy is still the gold standard for cancer confirmation.
What the Technology Does: From Phone Images to Pattern Recognition
AI skin-cancer detection often uses machine learning, a form of computer modelling that learns patterns from examples rather than from human-defined rules. Most systems today use convolutional neural networks, or CNN, which are deep learning models that analyse the images by identifying visual qualities such as edges, colours, shapes, textures and borders of lesions. In dermatology, these algorithms are trained on clinical photos, dermoscopic pictures or both and then tested on new images to predict if a lesion seems more benign or more concerning.
A phone can aid in two ways. At the most basic level, a smartphone camera may capture a conventional clinical image of a mole or skin lesion. In more advanced systems, the phone is linked with a dermoscopic attachment that increases magnification and lighting, producing a more clinically useful image for the AI.
That matters because a consumer phone snap in poor illumination is not the same as a standardized dermoscopic image taken in a clinic.
Some AI systems give a risk category like low risk or suspicious. Others provide a probability score, a triage recommendation or a referral request. These outputs are not a diagnosis. The risk score implies that the algorithm has identified certain features in the image that it has learned to associate with cancer on its training and validation data but does not imply that cancer is present. In clinical practice, the safest use of AI is frequently “augmented intelligence,” where the software supports but does not replace the clinician’s judgment.
Elastic scattering spectroscopy is a comparable but separate technique that looks at how light is scattered by tissue structures. This is not a normal photo app for your phone. Using a hand-held optical device and AI-enabled software, the system assesses the physical properties of a concerning lesion. This distinction concerns because proof and regulatory approval for a clinician-use optical equipment should not automatically carry over to unregulated phone apps used by the public.
Evidence and Real-World Meaning
There is interesting but spotty data for AI in skin-cancer detection. Early landmark research showed that deep-learning systems could classify photographs of skin cancer to the same level as dermatologists using controlled image datasets. But controlled databases are not the real-world clinic. Some cancers come in strange ways or in hard-to-photograph bodily areas.
A 2024 comprehensive review and meta-analysis in npj Digital Medicine contained 53 studies of which 19 were included in quantitative meta-analysis. The sensitivity and specificity across all clinician categories for AI algorithms were 87.0% and 77.1% respectively, compared to 79.78% and 73.6% for clinicians in general.
Sensitivity is defined as the ability to correctly identify disease when disease is present, and specificity is defined as the ability to correctly identify non-disease when cancer is not present. The same review concluded AI was clinically similar to professional dermatologists but warned that most studies were not prospective real-world trials.
In a 2026 extensive study in JAMA Dermatology, only prospective dermoscopy studies were included. In 11 prospective studies with >2,500 patients, pooled sensitivity was 80.9% and specificity 75.6% for AI alone and 78.6% and 75.2% for dermatologists. One AI-assisted dermatology study reported 91.9% sensitivity and 83.7% specificity [30].
It seems that collaboration between humans and AI can be more advantageous than AI only. The main problem was the small, varied evidence base (risk of bias).
A very pertinent phone-based study was a multicenter prospective diagnostic trial published in The Lancet Digital Health in 2023. It assessed AI with a cell phone and a simple optical link in patients with probable pigmented lesions. The diagnosis trial included 172 concerning pigmented lesions in 124 patients, of whom 84 were malignant, while the management research included 5,696 pigmented lesions in 66 high-risk patients. In diagnosis, a new seven-class AI system performed as well as specialists and better than less-experienced clinicians, but worse than specialists in treatment-management decisions.
This is a crucial distinction, as identifying a worrying pattern is not the same as deciding whether to biopsy, monitor, reassure or refer quickly.
Regulatory research also illustrates the importance of the phrase.* In January 2024, the U.S. Food and Drug Administration granted De Novo designation to a clinician-use AI-enabled device to treat concerning lesions suggestive of melanoma, basal cell carcinoma or squamous cell carcinoma in patients 40 years of age and older. The gadget is meant to be used by non-dermatologist physicians and should be used only when a lesion has been already identified as worrying*. According to the FDA indication, it should not be used as a screening tool, a single diagnostic criterion or a method to confirm skin cancer. In other words, a controlled technology is a supplement to clinical diagnosis, not a substitute for it.
Exciting post-authorization clinical results for this optical AI technology also shows trade-offs. The DERM-SUCCESS validation investigation included 1,005 people and 1,579 lesions at 22 primary care facilities, identifying 224 skin cancers. The sensitivity was roughly 96 percent, and the negative predictive value was approximately 97 percent, therefore a negative result was usually reassuring in the population studied. However, specificity was low implying that numerous benign lesions may be detected for further investigation. While this trade-off may be acceptable for a triage tool not to miss cancer, it can lead to more referrals, biopsies, expense and patient anxiety.
Limitations, Risks, and Unanswered Questions
The biggest problem is the false confidence. A false negative occurs when an AI software misclassifies a cancerous lesion as low risk or benign. This is therapeutically relevant in skin cancer as a delayed diagnosis of melanoma may mean fewer treatment options. The most worrisome are apps with a consumer interface that cause individuals to delay medical assessment after a comforting result. A safe AI system is not just about accuracy in a study, but how it changes patient behaviour in the real world.
Another risk is false positives. A false positive occurs when an AI tool flags a benign tumor as suspicious; more sensitivity generally results in lower specificity with more referral of benign lesions for biopsy or excision. This matters because biopsies cause scarring, cost, anxiety and unnecessary clinical workload. In a limited-access dermatological health system, too many false positives could make it harder for those who actually need urgent care to acquire appointments.
Bias is another huge concern. The performance of dermatological AI systems is influenced by the quality of datasets used to train and validate them. The algorithm may be less successful on groups with under-represented photographs of darker skin tones, acral sites (palms and soles), odd lesions or rare cancers. The investigations have employed a number of dermatology photo databases. Some AI models have struggled with rare illnesses and dark skin tones. This is significant because the diagnosis of skin cancer can be delayed in those with darker skin and an imbalanced AI tool could exacerbate an existing disparity.
Image quality is really a practical limitation. Factors like unclear cell phone image, poor lighting, shadows, hair, skin markings, compression artifacts and unequal distance from the lesion impair the performance of the algorithm. The clinical metadata also count. Metadata contains information not connected to the image, such as age, immunological condition, history of skin cancer, duration of lesion, symptoms, anatomical location, if the lesion is changing. A doctor can fill in those details, many image-only AI systems cannot.
Privacy and implementation need attention. Skin photos are medical data and certain images may reveal body location, identity or sensitive health information. AI systems working on the phone should have secure storage, transparent consent, cybersecurity precautions and clear constraints on how images are used to construct algorithms. Workflow design is also critical for health systems, as an AI advice is only meaningful if it links patients to rapid clinical assessment, dermoscopy, biopsy or reassurance when appropriate.
Conclusion
AI in dermatology is becoming beneficial clinically, but the safest interpretation is conservative and specific: a phone may help to take skin photographs and AI may help to identify lesions that need medical attention, especially with dermoscopy, standardized imaging and human oversight. It cannot diagnose skin cancer and should not be used to ignore a lesion that is changing, bleeding, painful, unusual or not healing.
The future will likely be human-led and AI-enabled. AI could support non-dermatology health care personnel in deciding if the lesions of concern should be sent to a specialist in general care. AI has the potential to help with the interpretation of dermoscopy and to mitigate the diversity in interpretation amongst specialists in care. Robustly verified phone-based solutions could assist direct patients more rapidly to the right level of treatment in public health. The boundary between good innovation and bad overreach will be a matter of validation, legislation, equity, clinical workflow and honest communication about what AI can and cannot do.
Evidence Rating
Mixed or limited evidence. AI systems for skin-cancer detection are grounded in image-classification research, several systematic reviews, growing prospective data, and at least one FDA-classified supplemental device for physician use. However, independent phone-based self-diagnosis evidence remains limited, consumer apps are highly heterogeneous, many studies are retrospective or done in selected settings, and concerns remain about false negatives, false positives, skin-tone bias, image quality, and real-world clinical outcomes.
Educational Disclaimer
This article is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Any suspicious, changing, bleeding, painful, rapidly growing, or non-healing skin lesion should be assessed by a qualified healthcare professional.
References
- Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2026. CA: A Cancer Journal for Clinicians. 2026. doi:10.3322/caac.70043
- U.S. Preventive Services Task Force. Skin Cancer: Screening. Recommendation Statement. 2023.
- Esteva A, Kuprel B, Novoa RA, et al. Dermatologist-level classification of skin cancer with deep neural networks. Nature. 2017;542:115–118. doi:10.1038/nature21056
- Dinnes J, Deeks JJ, Chuchu N, et al. Smartphone applications for triaging adults with skin lesions that are suspicious for melanoma. Cochrane Database of Systematic Reviews. 2018;12.
- Jones OT, Matin RN, van der Schaar M, et al. Artificial intelligence and machine learning algorithms for early detection of skin cancer in community and primary care settings: a systematic review. The Lancet Digital Health. 2022;4(6)–e476. doi:10.1016/S2589-7500(22)00023-1
- Salinas MP, Sepúlveda J, Hidalgo L, et al. A systematic review and meta-analysis of artificial intelligence versus clinicians for skin cancer diagnosis. npj Digital Medicine. 2024;7:125. doi:10.1038/s41746-024-01103-x
- Laiouar-Pedari S, Kühn A, Wies C, et al. Prospective Evidence on Artificial Intelligence–Assisted Melanoma Diagnostics: A Systematic Review and Meta-Analysis. JAMA Dermatology. 2026;162(5):478–487. doi:10.1001/jamadermatol.2026.0217
- Menzies SW, Sinz C, Menzies M, et al. Comparison of humans versus mobile phone-powered artificial intelligence for the diagnosis and management of pigmented skin cancer in secondary care: a multicentre, prospective, diagnostic, clinical trial. The Lancet Digital Health. 2023;5(10)–e691. doi:10.1016/S2589-7500(23)00130-9
- U.S. Food and Drug Administration. De Novo Classification Request DEN230008: DermaSensor. Decision date January 12, 2024.
- Manolakos D, Patrick G, Geisse JK, et al. Use of an elastic-scattering spectroscopy and artificial intelligence device in the assessment of lesions suggestive of skin cancer: a comparative effectiveness study. JAAD International. 2024;14:52–58. doi:10.1016/j.jdin.2023.08.019
- Merry SP, Croghan IT, Dukes KA, et al. Primary Care Physician Use of Elastic Scattering Spectroscopy on Skin Lesions Suggestive of Skin Cancer. Journal of Primary Care & Community Health. 2025;16:21501319251344423. doi:10.1177/21501319251344423
- Ferris LK, Jaklitsch E, Seiverling EV, et al. DERM-SUCCESS FDA Pivotal Study: A Multi-Reader Multi-Case Evaluation of Primary Care Physicians’ Skin Cancer Detection Using AI-Enabled Elastic Scattering Spectroscopy. Journal of Primary Care & Community Health. 2025;16:21501319251342106. doi:10.1177/21501319251342106
- Daneshjou R, Vodrahalli K, Novoa RA, et al. Disparities in dermatology AI performance on a diverse, curated clinical image set. Science Advances. 2022;8(31). doi:10.1126/sciadv.abq6147
- American Academy of Dermatology. Teledermatology Standards.